You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- TM 9-1751 Cylinder, Radial, Gasoline Engine (Continental Model R975-C1) 1944Document237 pagesTM 9-1751 Cylinder, Radial, Gasoline Engine (Continental Model R975-C1) 1944Kelsey Yuen50% (2)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- 01 - Accounting For Managers PDFDocument151 pages01 - Accounting For Managers PDFAmit Kumar PandeyNo ratings yet
- Poka Yoke BDocument31 pagesPoka Yoke BjaymuscatNo ratings yet
- Marcel Breuer: Hungarian-American Designer, Architect and Bauhaus PioneerDocument8 pagesMarcel Breuer: Hungarian-American Designer, Architect and Bauhaus PioneerYosaphat Kiko Paramore DiggoryNo ratings yet
- Evoked PotentialsDocument49 pagesEvoked PotentialsparuNo ratings yet
- Electrical Power System Design For Industrial FacilitiesDocument29 pagesElectrical Power System Design For Industrial Facilitiesgusgon521292100% (1)
- Banking Finance Agile TestingDocument4 pagesBanking Finance Agile Testinganil1karnatiNo ratings yet
- Draft Horse Primer Guide To Care Use of Work Horses and Mules 1977Document396 pagesDraft Horse Primer Guide To Care Use of Work Horses and Mules 1977Radu IliescuNo ratings yet
- OilField Review 2016 Cement EvaluationDocument10 pagesOilField Review 2016 Cement EvaluationLuisNo ratings yet
- Final Mother DairyDocument59 pagesFinal Mother DairyAnup Dcruz100% (4)
- Q.850 ISDN Cause CodesDocument12 pagesQ.850 ISDN Cause CodesJack CastineNo ratings yet
- SSTMCV Retail PowerDocument5 pagesSSTMCV Retail Powervipin.yadavNo ratings yet
- New England Journal Medicine: The ofDocument10 pagesNew England Journal Medicine: The ofTiffany Rachma PutriNo ratings yet
- Ocuplasi BurnDocument9 pagesOcuplasi BurnUtomo FemtomNo ratings yet
- UveitisDocument10 pagesUveitisUtomo FemtomNo ratings yet
- FentanylDocument12 pagesFentanylUtomo FemtomNo ratings yet
- Bjorl: Clinical and Functional Aspects of Body Balance in Elderly Subjects With Benign Paroxysmal Positional VertigoDocument8 pagesBjorl: Clinical and Functional Aspects of Body Balance in Elderly Subjects With Benign Paroxysmal Positional VertigoUtomo FemtomNo ratings yet
- Tetanus: Pembimbing: Dr. Subandi, SP.S (K), FINACSDocument27 pagesTetanus: Pembimbing: Dr. Subandi, SP.S (K), FINACSUtomo FemtomNo ratings yet
- Contemporary Clinical Trials: Natalia A. Ricci, Mayra C. Aratani, Heloísa H. Caovilla, Fernando F. GanançaDocument9 pagesContemporary Clinical Trials: Natalia A. Ricci, Mayra C. Aratani, Heloísa H. Caovilla, Fernando F. GanançaUtomo FemtomNo ratings yet
- CKD Dengan DislipidemiaDocument9 pagesCKD Dengan DislipidemiaUtomo FemtomNo ratings yet
- Efikasi Dan Tolerabilitas Lamotrigin Di Juvenile Mioklonik Epilepsi Pada Orang DewasaDocument10 pagesEfikasi Dan Tolerabilitas Lamotrigin Di Juvenile Mioklonik Epilepsi Pada Orang DewasaUtomo FemtomNo ratings yet
- Komplikasi CKDDocument6 pagesKomplikasi CKDUtomo FemtomNo ratings yet
- CKD & DiabetesDocument9 pagesCKD & DiabetesUtomo FemtomNo ratings yet
- Kelangsungan Hidup Fungsional Setelah Perawatan Akut Untuk Cedera Kepala Berat Di Sebuah Pusat Trauma Yang Ditunjuk Di Hong KongDocument6 pagesKelangsungan Hidup Fungsional Setelah Perawatan Akut Untuk Cedera Kepala Berat Di Sebuah Pusat Trauma Yang Ditunjuk Di Hong KongUtomo FemtomNo ratings yet
- Pemberian Aspirin Dengan CKDDocument10 pagesPemberian Aspirin Dengan CKDUtomo FemtomNo ratings yet
- CKD Dengan DislipidemiaDocument9 pagesCKD Dengan DislipidemiaUtomo FemtomNo ratings yet
- Pemberian Simvastatin Pada CKDDocument12 pagesPemberian Simvastatin Pada CKDUtomo FemtomNo ratings yet
- Daya Tahan Endovascular Melingkar Dibandingkan Pembedahan Kliping Aneurisma Otak PecahDocument7 pagesDaya Tahan Endovascular Melingkar Dibandingkan Pembedahan Kliping Aneurisma Otak PecahUtomo FemtomNo ratings yet
- Renal Manometers Pada CKDDocument6 pagesRenal Manometers Pada CKDUtomo FemtomNo ratings yet
- Daya Tahan Endovascular Melingkar Dibandingkan Pembedahan Kliping Aneurisma Otak PecahDocument7 pagesDaya Tahan Endovascular Melingkar Dibandingkan Pembedahan Kliping Aneurisma Otak PecahUtomo FemtomNo ratings yet
- Komplikasi CKDDocument6 pagesKomplikasi CKDUtomo FemtomNo ratings yet
- Akut Sakit Kepala Di Departemen DaruratDocument8 pagesAkut Sakit Kepala Di Departemen DaruratUtomo FemtomNo ratings yet
- Perbandingan Hipotermia Dan Normothermia Setelah Cedera Otak Traumatik Parah Pada Anak-Anak LDocument8 pagesPerbandingan Hipotermia Dan Normothermia Setelah Cedera Otak Traumatik Parah Pada Anak-Anak LUtomo FemtomNo ratings yet
- Pemberian Simvastatin Pada CKDDocument12 pagesPemberian Simvastatin Pada CKDUtomo FemtomNo ratings yet
- Tugs DR - IpulDocument5 pagesTugs DR - IpulUtomo FemtomNo ratings yet
- Perbandingan Hipotermia Dan Normothermia Setelah Cedera Otak Traumatik Parah Pada Anak-Anak LDocument8 pagesPerbandingan Hipotermia Dan Normothermia Setelah Cedera Otak Traumatik Parah Pada Anak-Anak LUtomo FemtomNo ratings yet
- Daya Tahan Endovascular Melingkar Dibandingkan Pembedahan Kliping Aneurisma Otak PecahDocument7 pagesDaya Tahan Endovascular Melingkar Dibandingkan Pembedahan Kliping Aneurisma Otak PecahUtomo FemtomNo ratings yet
- Akut Sakit Kepala Di Departemen DaruratDocument8 pagesAkut Sakit Kepala Di Departemen DaruratUtomo FemtomNo ratings yet
- 1 s2.0 S0091674914000633Document13 pages1 s2.0 S0091674914000633Utomo FemtomNo ratings yet
- Pemberian Simvastatin Pada CKDDocument12 pagesPemberian Simvastatin Pada CKDUtomo FemtomNo ratings yet
- Pemberian Aspirin Dengan CKDDocument10 pagesPemberian Aspirin Dengan CKDUtomo FemtomNo ratings yet
- CKD & DiabetesDocument9 pagesCKD & DiabetesUtomo FemtomNo ratings yet
- TT1 2lecture SpinningDocument29 pagesTT1 2lecture SpinninghaiNo ratings yet
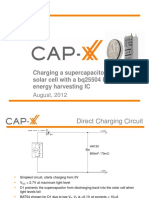
- 1208 CAP XX Charging A Supercapacitor From A Solar Cell PDFDocument12 pages1208 CAP XX Charging A Supercapacitor From A Solar Cell PDFmehralsmenschNo ratings yet
- Norlys 2016Document124 pagesNorlys 2016elektrospecNo ratings yet
- Banking Software System Monitoring ToolDocument4 pagesBanking Software System Monitoring ToolSavun D. CheamNo ratings yet
- Block P2P Traffic with pfSense using Suricata IPSDocument6 pagesBlock P2P Traffic with pfSense using Suricata IPSEder Luiz Alves PintoNo ratings yet
- Alcalel-Lucent WLAN OmniAcces StellarDocument6 pagesAlcalel-Lucent WLAN OmniAcces StellarJBELDNo ratings yet
- Loctite 270™: Technical Data SheetDocument4 pagesLoctite 270™: Technical Data SheetM Jobayer AzadNo ratings yet
- Less Than a Decade to Avoid Catastrophic Climate ChangeDocument1 pageLess Than a Decade to Avoid Catastrophic Climate ChangeXie YuJiaNo ratings yet
- Understanding Nominal Pipe Sizes (NPS) and Pipe DimensionsDocument39 pagesUnderstanding Nominal Pipe Sizes (NPS) and Pipe DimensionsprathikNo ratings yet
- CLS1Document3 pagesCLS1Shaina Kaye De GuzmanNo ratings yet
- 489-F Latest JudgmentDocument15 pages489-F Latest JudgmentMoving StepNo ratings yet
- Gray Cast Iron Stress ReliefDocument25 pagesGray Cast Iron Stress ReliefSagarKBLNo ratings yet
- MunnarDocument5 pagesMunnarvisujinuNo ratings yet
- Đề Số 1 - Đề Phát Triển Đề Minh Họa 2023Document20 pagesĐề Số 1 - Đề Phát Triển Đề Minh Họa 2023Maru KoNo ratings yet
- Service Manual: DCR-DVD150E/DVD450E/DVD650/ DVD650E/DVD850/DVD850EDocument71 pagesService Manual: DCR-DVD150E/DVD450E/DVD650/ DVD650E/DVD850/DVD850EJonathan Da SilvaNo ratings yet
- Depreciation Methods ExplainedDocument2 pagesDepreciation Methods ExplainedAnsha Twilight14No ratings yet
- Green Ecobuses Run On This Route.: BusesDocument6 pagesGreen Ecobuses Run On This Route.: BusesLuis DíazNo ratings yet
- Guidelines Regarding The Handling of Cable Drums During Transport and StorageDocument5 pagesGuidelines Regarding The Handling of Cable Drums During Transport and StorageJegan SureshNo ratings yet