You might also like
- Pro 3 Cases - Long and ShortDocument6 pagesPro 3 Cases - Long and ShortKalichandren ArumugamNo ratings yet
- GDocument17 pagesGKalichandren ArumugamNo ratings yet
- SKILL LAB-HWS Relax TechniqueDocument2 pagesSKILL LAB-HWS Relax TechniqueKalichandren ArumugamNo ratings yet
- PresentationDocument1 pagePresentationAlexandra NeculaiNo ratings yet
- EPSON L210 Series Advanced Driver SettingsDocument1 pageEPSON L210 Series Advanced Driver SettingsKalichandren ArumugamNo ratings yet
- ClinicoSocial Case on Household Assets and SanitationDocument9 pagesClinicoSocial Case on Household Assets and SanitationKalichandren ArumugamNo ratings yet
- International Medical SchoolDocument1 pageInternational Medical SchoolKalichandren ArumugamNo ratings yet
- PresentationDocument1 pagePresentationAlexandra NeculaiNo ratings yet
- Year 3 October Intake - Rot 4time Table, 2015Document11 pagesYear 3 October Intake - Rot 4time Table, 2015Kalichandren ArumugamNo ratings yet
- MnemonicDocument21 pagesMnemonicWiDya EmiLiaNo ratings yet
- Presentation 4Document11 pagesPresentation 4Kalichandren ArumugamNo ratings yet
- Year 3 October Intake - Rot 4time Table, 2015Document11 pagesYear 3 October Intake - Rot 4time Table, 2015Kalichandren ArumugamNo ratings yet
- Att List Mbbs Year 3 - Theory (5 June)Document176 pagesAtt List Mbbs Year 3 - Theory (5 June)Kalichandren ArumugamNo ratings yet
- Title Layout: SubtitleDocument11 pagesTitle Layout: SubtitleKalichandren ArumugamNo ratings yet
- 2Document17 pages2Kalichandren ArumugamNo ratings yet
- Respi SystemDocument6 pagesRespi SystemKalichandren ArumugamNo ratings yet
- EPSON L210 Series Advanced Driver SettingsDocument1 pageEPSON L210 Series Advanced Driver SettingsKalichandren ArumugamNo ratings yet
- Spiro Me TryDocument22 pagesSpiro Me TryKalichandren ArumugamNo ratings yet
- Year 3 - Learning OutcomeDocument8 pagesYear 3 - Learning OutcomeKalichandren ArumugamNo ratings yet
- Spiro Me TryDocument22 pagesSpiro Me TryKalichandren ArumugamNo ratings yet
- CPG Management of Type 2 Diabetes Mellitus (4th Edition)Document84 pagesCPG Management of Type 2 Diabetes Mellitus (4th Edition)apalaginih100% (3)
- CPG Medical StudentsDocument33 pagesCPG Medical StudentsKalichandren ArumugamNo ratings yet
- Chapter 71: Acute Gastroenteritis: Is The Child in Shock? Any Child With Shock Go Straight To Treatment Plan CDocument7 pagesChapter 71: Acute Gastroenteritis: Is The Child in Shock? Any Child With Shock Go Straight To Treatment Plan CKalichandren ArumugamNo ratings yet
- Chest PainDocument7 pagesChest PainKalichandren ArumugamNo ratings yet
- CardiovascularDocument8 pagesCardiovascularHampson MalekanoNo ratings yet
- CP 4Document79 pagesCP 4Kalichandren ArumugamNo ratings yet
- Chapter 71: Acute Gastroenteritis: Is The Child in Shock? Any Child With Shock Go Straight To Treatment Plan CDocument5 pagesChapter 71: Acute Gastroenteritis: Is The Child in Shock? Any Child With Shock Go Straight To Treatment Plan CKalichandren ArumugamNo ratings yet
- Forcep SeminarDocument3 pagesForcep SeminarKalichandren ArumugamNo ratings yet
- Groupon 4FA0D9B6F7Document1 pageGroupon 4FA0D9B6F7Kalichandren ArumugamNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Ficha Tecnica StyrofoamDocument2 pagesFicha Tecnica StyrofoamAceroMart - Tu Mejor Opcion en AceroNo ratings yet
- 6.water Treatment and Make-Up Water SystemDocument18 pages6.water Treatment and Make-Up Water Systempepenapao1217100% (1)
- Rawat Inap Rumah Sakit Santa Elisabeth Medan Englin Moria K. Tinambunan, Lindawati F. Tampubolon, Erika E. SembiringDocument14 pagesRawat Inap Rumah Sakit Santa Elisabeth Medan Englin Moria K. Tinambunan, Lindawati F. Tampubolon, Erika E. SembiringafrilianaNo ratings yet
- Treating Thyroid Emergencies: Myxedema Coma and Thyroid StormDocument17 pagesTreating Thyroid Emergencies: Myxedema Coma and Thyroid StormMarlon UlloaNo ratings yet
- Lesson 8 - Philippine Disaster Risk Reduction and Management SystemDocument11 pagesLesson 8 - Philippine Disaster Risk Reduction and Management SystemMary Joy CuetoNo ratings yet
- ĐỀ THI THU TNTHPT SỐ 17Document4 pagesĐỀ THI THU TNTHPT SỐ 17Nguyên Hà NguyễnNo ratings yet
- Naskah PublikasiDocument14 pagesNaskah PublikasiNirmala malaNo ratings yet
- Presentation On Data Integrity in PharmaDocument80 pagesPresentation On Data Integrity in Pharmaskvemula67% (3)
- Adolescent and Sexual HealthDocument36 pagesAdolescent and Sexual Healthqwerty123No ratings yet
- BOD FormatDocument4 pagesBOD FormatSkill IndiaNo ratings yet
- Corn Pulao Recipe With Sweet CornDocument2 pagesCorn Pulao Recipe With Sweet CornSudharshanNo ratings yet
- Ethnobotany Manual 14th September 2016Document54 pagesEthnobotany Manual 14th September 2016Rahul0% (1)
- The Motive Journal (3rd Edition)Document42 pagesThe Motive Journal (3rd Edition)Shubham Sharma0% (1)
- Abnegation Faction:: Clothing Is Gray and Simple. The OnlyDocument7 pagesAbnegation Faction:: Clothing Is Gray and Simple. The OnlylethaagathaNo ratings yet
- Healthcare Financing in IndiADocument86 pagesHealthcare Financing in IndiAGeet Sheil67% (3)
- Density of Aggregates: ObjectivesDocument4 pagesDensity of Aggregates: ObjectivesKit Gerald EliasNo ratings yet
- VentilationDocument92 pagesVentilationRobert Nixon100% (1)
- CanteenDocument8 pagesCanteenmahesh4uNo ratings yet
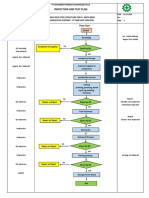
- Inspection and Test Plan: Flow Chart Start IncomingDocument1 pageInspection and Test Plan: Flow Chart Start IncomingSinden AyuNo ratings yet
- Bandong 3is Q4M6Document6 pagesBandong 3is Q4M6Kento RyuNo ratings yet
- Piaggio MP3 300 Ibrido LT MY 2010 (En)Document412 pagesPiaggio MP3 300 Ibrido LT MY 2010 (En)Manualles100% (3)
- RJ Bensingh Pub Composites CoatingsDocument5 pagesRJ Bensingh Pub Composites CoatingsFakkir MohamedNo ratings yet
- Methodology For The Validation of Fuel Consumption in Diesel Engines Installed On Board Military Ships, Using Diesel Oil and Biodiesel BlendsDocument16 pagesMethodology For The Validation of Fuel Consumption in Diesel Engines Installed On Board Military Ships, Using Diesel Oil and Biodiesel BlendsErick RodriguesNo ratings yet
- Restaurant Supervisor Job Description Job SummaryDocument3 pagesRestaurant Supervisor Job Description Job SummaryKumarSvNo ratings yet
- CWK-IDD-009-CC-2020: Reference Checking Consent and Authorization Form Candidate's Full NameDocument1 pageCWK-IDD-009-CC-2020: Reference Checking Consent and Authorization Form Candidate's Full NamePopa Alina-ManuelaNo ratings yet
- 4Document130 pages4Upender BhatiNo ratings yet
- Jamec Air FittingsDocument18 pagesJamec Air Fittingsgoeez1No ratings yet
- Fischer FBN II BoltDocument5 pagesFischer FBN II BoltJaga NathNo ratings yet
- Product GuideDocument13 pagesProduct Guidekhalid mostafaNo ratings yet
- Chin Cup Therapy An Effective Tool For The Correction of Class III Malocclusion in Mixed and Late Deciduous DentitionsDocument6 pagesChin Cup Therapy An Effective Tool For The Correction of Class III Malocclusion in Mixed and Late Deciduous Dentitionschic organizerNo ratings yet