You might also like
- Pre-eclampsia, (Pregnancy with Hypertension And Proteinuria) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPre-eclampsia, (Pregnancy with Hypertension And Proteinuria) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Abruptio Placenta: Prepared By: Claire Alvarez Ongchua, RNDocument42 pagesAbruptio Placenta: Prepared By: Claire Alvarez Ongchua, RNclaireaongchua1275100% (2)
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Hydatifor M Mole: By: Namita Arya Asst. Lecturer PDMSNCDocument27 pagesHydatifor M Mole: By: Namita Arya Asst. Lecturer PDMSNCnamitaNo ratings yet
- GTD Case StudyDocument9 pagesGTD Case StudyZnarf Izlah Sadanreb100% (1)
- Biophysical Profile PDFDocument1 pageBiophysical Profile PDFmp1757No ratings yet
- Placenta PreviaDocument33 pagesPlacenta PreviaAcohCChao100% (1)
- Postpartum AssessmentDocument3 pagesPostpartum AssessmentgirishNo ratings yet
- PihDocument35 pagesPihmark100% (6)
- Labor Delivery Nursing 1209267990824369 9Document72 pagesLabor Delivery Nursing 1209267990824369 9Jay Depakakibo Gallardo100% (1)
- Gestational Diabetes Mellitus (GDM)Document26 pagesGestational Diabetes Mellitus (GDM)Chrizzia Del RosarioNo ratings yet
- Placenta AbruptioDocument30 pagesPlacenta AbruptioArchana MaharjanNo ratings yet
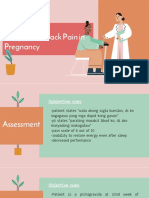
- Fatigue and Back Pain NCP PresentationDocument18 pagesFatigue and Back Pain NCP PresentationTine Guibao100% (1)
- Abruptio PlacentaDocument8 pagesAbruptio PlacentaNutz TolentinoNo ratings yet
- Hydatidiform Mole - OverviewDocument4 pagesHydatidiform Mole - Overviewannmanalad9438No ratings yet
- Case Study Presentation: Group 2Document12 pagesCase Study Presentation: Group 2Anna Marie Donaire0% (1)
- Pyloric StenosisDocument5 pagesPyloric Stenosisensoooooooooo100% (1)
- Abruptio PlacentaDocument5 pagesAbruptio PlacentaJuan Carlo Z. SolidumNo ratings yet
- 16 Amniotic Fluid EmbolismDocument46 pages16 Amniotic Fluid EmbolismAhmed TarigNo ratings yet
- Incompetent CervixDocument5 pagesIncompetent CervixNaidin Catherine De Guzman-Alcala100% (1)
- Hyper Emesis GravidarumDocument22 pagesHyper Emesis Gravidarumchandu ranaNo ratings yet
- Case Pres AutosavedDocument21 pagesCase Pres AutosavedJaysellePuguonTabijeNo ratings yet
- Cesarean SectionDocument61 pagesCesarean SectionDaniel Ramos GomezNo ratings yet
- Pre Eclampsia - FinalDocument54 pagesPre Eclampsia - Finalsupernurse02No ratings yet
- Unit VIII PRESUMPTIVE SIGNS AND SYMPTOMS OF PREGNANCYDocument5 pagesUnit VIII PRESUMPTIVE SIGNS AND SYMPTOMS OF PREGNANCYNancy100% (1)
- Assessment of NewbornDocument26 pagesAssessment of Newbornaybee_14No ratings yet
- Process of LabourDocument6 pagesProcess of LabourAnnapurna Dangeti100% (1)
- Complications During Labor and Delivery - HardDocument19 pagesComplications During Labor and Delivery - Hardkrizele ann santosNo ratings yet
- Abnormal Progress in Labor (Precipitous Labor and Birth & Retraction Rings)Document34 pagesAbnormal Progress in Labor (Precipitous Labor and Birth & Retraction Rings)Ana100% (3)
- A Case Report On Multifetal PregnancyDocument5 pagesA Case Report On Multifetal PregnancyThreecee VelezNo ratings yet
- Birth Asphyxia: by Anne E. Odaro MCM/2017/69852Document26 pagesBirth Asphyxia: by Anne E. Odaro MCM/2017/69852ElvisNo ratings yet
- Drugs - OBDocument7 pagesDrugs - OBglennarthurNo ratings yet
- Vacuum Extraction (Ventouse)Document3 pagesVacuum Extraction (Ventouse)dusty kawiNo ratings yet
- Retained Placenta-OB Shock-Uterine InversionDocument38 pagesRetained Placenta-OB Shock-Uterine InversionBien Bosito0% (1)
- Assessment Nsg. Diagnosis Sci. Explanation Planning Intervention Rationale EvaluationDocument6 pagesAssessment Nsg. Diagnosis Sci. Explanation Planning Intervention Rationale EvaluationRoMarie AbainzaNo ratings yet
- Placenta PreviaDocument11 pagesPlacenta PreviaHomerNo ratings yet
- Placenta Previa TotalisDocument34 pagesPlacenta Previa TotalisRujira Angkinan100% (4)
- Multifetal Pregnancy: Amr Nadim, MDDocument36 pagesMultifetal Pregnancy: Amr Nadim, MDsharenNo ratings yet
- Care Study - CholedocholithiasisDocument29 pagesCare Study - CholedocholithiasisNehdu AkahNo ratings yet
- A Case Presentation On CholedocholithiasisDocument11 pagesA Case Presentation On CholedocholithiasisPaul Vincent EspereNo ratings yet
- Abruptio PlacentaDocument29 pagesAbruptio PlacentaAudrey DelfinNo ratings yet
- Case Study CholecystitisDocument33 pagesCase Study CholecystitisMelai de GuzmanNo ratings yet
- Mechanism of LaborDocument12 pagesMechanism of LaborSaidatul Safarah Md HassanNo ratings yet
- HyperbilirubinemiaDocument11 pagesHyperbilirubinemianursereview100% (12)
- NCM - Pregancy Induced HypertensionDocument5 pagesNCM - Pregancy Induced HypertensionZam PamateNo ratings yet
- Care PlanDocument4 pagesCare PlangopscharanNo ratings yet
- Nursing Care Plan General Objective: To Promote Safety Through Prevention of The Spread of InfectionDocument3 pagesNursing Care Plan General Objective: To Promote Safety Through Prevention of The Spread of InfectionitsmeayaNo ratings yet
- Gestational Diabetes Mellitus PDFDocument7 pagesGestational Diabetes Mellitus PDFMaxenia FaboresNo ratings yet
- Fetal DistressDocument32 pagesFetal DistressMadhu Sudhan PandeyaNo ratings yet
- Gestational Diabetes: Dr. Oyeyiola Oyebode Registrar Obstetrics and Gynaecology Ola Catholic Hospital, Oluyoro IbadanDocument40 pagesGestational Diabetes: Dr. Oyeyiola Oyebode Registrar Obstetrics and Gynaecology Ola Catholic Hospital, Oluyoro Ibadanoyebode oyeyiolaNo ratings yet
- Conducting A Normal DeliveryDocument26 pagesConducting A Normal DeliveryRedroses flowersNo ratings yet
- Post Partum HemorrhageDocument40 pagesPost Partum HemorrhageGita GirsangNo ratings yet
- HMOLEDocument34 pagesHMOLEZuellen Mae Garapan BedañoNo ratings yet
- Diabetes in PregnancyDocument88 pagesDiabetes in PregnancyKathleenZunigaNo ratings yet
- Uterine ProlapseDocument11 pagesUterine ProlapseMelDred Cajes BolandoNo ratings yet
- Case Study PreeclampsiaDocument3 pagesCase Study PreeclampsiaRima Christa Ulin SitepuNo ratings yet
- NSDDocument44 pagesNSDabyssodeep100% (1)
- Hyperemesis GravidarumDocument31 pagesHyperemesis GravidarumFeregrine VerayoNo ratings yet
- EpisiotomyDocument18 pagesEpisiotomyAnnapurna DangetiNo ratings yet
- Late Pregnancy Bleeding: Kareem Ayman Sultan 200008Document67 pagesLate Pregnancy Bleeding: Kareem Ayman Sultan 200008200008No ratings yet
- Autonomic NotesDocument4 pagesAutonomic NotesYeyeth Jabaybay TabolongNo ratings yet
- Plysu People No.3 Autumn 1971Document8 pagesPlysu People No.3 Autumn 1971Richard LarbeyNo ratings yet
- Io Pet Person Sit Sleep Table Spec Document: !!!watch The Instructional Video Here!!!Document16 pagesIo Pet Person Sit Sleep Table Spec Document: !!!watch The Instructional Video Here!!!Carlos CastroNo ratings yet
- Exercise Unit 3 - HomophonesDocument2 pagesExercise Unit 3 - HomophonesEmmot LizawatiNo ratings yet
- City of BonesDocument28 pagesCity of BonesScribd_TJ58% (12)
- The International Customs JournalDocument495 pagesThe International Customs Journaldrin_kaNo ratings yet
- Psoas StretchesDocument9 pagesPsoas Stretcheswalterego58No ratings yet
- Straightforward Upper Intermediate Unit 2 Test: Name - Score - /50Document3 pagesStraightforward Upper Intermediate Unit 2 Test: Name - Score - /50Velichka IvanovaNo ratings yet
- Materi Siap Us Bahasa Inggris SMPN 1 SumobitoDocument3 pagesMateri Siap Us Bahasa Inggris SMPN 1 SumobitoYUNI HARTONO KHITDHYSNo ratings yet
- Cotton Count Yarn Size Conversion To Tex SizeDocument2 pagesCotton Count Yarn Size Conversion To Tex SizeZaheer_1994No ratings yet
- Geollegue-Angel-Dlp-English (Verb)Document3 pagesGeollegue-Angel-Dlp-English (Verb)Angel Licayan GeollegueNo ratings yet
- Diagram Shows The Human Breathing System.: Answer All The QuestionDocument14 pagesDiagram Shows The Human Breathing System.: Answer All The QuestionLori GonzalezNo ratings yet
- Lesson 2 - VerbsDocument6 pagesLesson 2 - VerbsAkbarul AminNo ratings yet
- Preparation of Soybean Milk and Its Comparison With Natural MilkDocument12 pagesPreparation of Soybean Milk and Its Comparison With Natural MilkHarsh BhdauriyaNo ratings yet
- SCIENCE 6 Summative Test #1 QTR 2Document4 pagesSCIENCE 6 Summative Test #1 QTR 2Jovelyn L. Lucio100% (1)
- Alicia Extended EndingDocument11 pagesAlicia Extended EndingtNo ratings yet
- Conditionals Type 2 Esl Multiple Choice Quiz For KidsDocument3 pagesConditionals Type 2 Esl Multiple Choice Quiz For KidsOrlando MotaNo ratings yet
- Bad Wrong Things A Best Friends Dad MM Romance (C.p. Harris)Document297 pagesBad Wrong Things A Best Friends Dad MM Romance (C.p. Harris)Fiorella Galván33% (3)
- Muscular System Tour Activity FormDocument19 pagesMuscular System Tour Activity Formmr_afmNo ratings yet
- 2 Step PPD FormDocument1 page2 Step PPD FormWilliamNo ratings yet
- Previous IB Exam QuestionsDocument12 pagesPrevious IB Exam QuestionsJohn OsborneNo ratings yet
- Recipes of CasserolesDocument7 pagesRecipes of CasserolesbhaleshNo ratings yet
- Advance Organizer Venn Diagram Linear and Nonlinear Texts Flow DiagramDocument7 pagesAdvance Organizer Venn Diagram Linear and Nonlinear Texts Flow Diagramjoshua rosillonNo ratings yet
- Animal Protect Themselves Folio Thanis 1Document25 pagesAnimal Protect Themselves Folio Thanis 1Kisor SorNo ratings yet
- Full Entry Test B2-C1-C2Document6 pagesFull Entry Test B2-C1-C2Cristina PupezaNo ratings yet
- Duck Duck and Her FriendsDocument6 pagesDuck Duck and Her FriendsAlexis De Leon100% (1)
- Course Review KeyDocument24 pagesCourse Review KeyHermann Dejero LozanoNo ratings yet
- Dallas Morning News PDF Version Page 1Document1 pageDallas Morning News PDF Version Page 1api-213784103No ratings yet
- BIO Notes Class 12Document14 pagesBIO Notes Class 12Marwa KhotNo ratings yet
- Animal NutritionDocument51 pagesAnimal NutritionknlsinhaNo ratings yet