You might also like
- Causes and Management of Syncope in DentistryDocument27 pagesCauses and Management of Syncope in DentistrySelvarathi KandhaswamyNo ratings yet
- Childhood Pneumonia Diagnosis and TreatmentDocument65 pagesChildhood Pneumonia Diagnosis and TreatmentYemata HailuNo ratings yet
- HypertensionDocument12 pagesHypertensionDr. PARMINDER NAINNo ratings yet
- SyncopeDocument28 pagesSyncopeDurgesh PushkarNo ratings yet
- Comatose PatientDocument126 pagesComatose PatientbrhomzalatNo ratings yet
- Myasthenia GravisDocument33 pagesMyasthenia GravisLovely Cervantes100% (1)
- Neurologicdisorders 100816033614 Phpapp01 PDFDocument96 pagesNeurologicdisorders 100816033614 Phpapp01 PDFenam professorNo ratings yet
- The Human Nervous Syste1Document10 pagesThe Human Nervous Syste1taytay321No ratings yet
- Types and Categories of PainDocument15 pagesTypes and Categories of Painpasser byNo ratings yet
- Approach To An Unconscious Patient-OyeyemiDocument41 pagesApproach To An Unconscious Patient-OyeyemiOyeyemi AdeyanjuNo ratings yet
- Asthma: A. DefinitionDocument6 pagesAsthma: A. DefinitionElvando SimatupangNo ratings yet
- InfluenzaDocument16 pagesInfluenzaTrue AlphaNo ratings yet
- Cranial Nerves Examination GuideDocument14 pagesCranial Nerves Examination GuideMoussa FarhatNo ratings yet
- Thyroid CrisisDocument11 pagesThyroid CrisisKoka KolaNo ratings yet
- Unit 1Document16 pagesUnit 1reeta yadav0% (1)
- Measuring and Understanding Blood PressureDocument44 pagesMeasuring and Understanding Blood PressureFarwaNo ratings yet
- Referred PainDocument3 pagesReferred PainaspalavistaNo ratings yet
- Slides For SeizureDocument15 pagesSlides For SeizureBryan Mae H. Degorio100% (3)
- Adverse Drug Reactions (ADRS)Document24 pagesAdverse Drug Reactions (ADRS)ANAM IQBALNo ratings yet
- CHF Drugs Guide: Key Medications for Treating Congestive Heart FailureDocument21 pagesCHF Drugs Guide: Key Medications for Treating Congestive Heart Failuremohsen mirdamadiNo ratings yet
- Brown Sequard SyndromeDocument7 pagesBrown Sequard SyndromeAiman RayyanNo ratings yet
- Calcium Homeostasis: Endocrine Regulation of (Ca)Document4 pagesCalcium Homeostasis: Endocrine Regulation of (Ca)PRANAB KUMAR MUKHERJEENo ratings yet
- Cardiovascular AccidentDocument7 pagesCardiovascular AccidentSHEILA MAE SACLOTNo ratings yet
- Approach To Comatose Child: DR G.VenkateshDocument83 pagesApproach To Comatose Child: DR G.VenkateshG VenkateshNo ratings yet
- Lower Respiratory Tract Infections: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingDocument95 pagesLower Respiratory Tract Infections: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingRI NANo ratings yet
- Chronic Suppurative Otitis MediaDocument11 pagesChronic Suppurative Otitis MediaaditiarrtuguNo ratings yet
- Mounika G1Document8 pagesMounika G1pandem soniyaNo ratings yet
- BreastDocument2 pagesBreastPretty UNo ratings yet
- Pain PathwaysDocument45 pagesPain PathwaysKabirNo ratings yet
- Premedication for Dental SurgeryDocument44 pagesPremedication for Dental Surgeryanjali sNo ratings yet
- TuberculomaDocument7 pagesTuberculomaAdeleNo ratings yet
- Amyotrophic Lateral SclerosisDocument15 pagesAmyotrophic Lateral Sclerosisyamie sulongNo ratings yet
- ARDS Care Respiratory Care Plan PDFDocument2 pagesARDS Care Respiratory Care Plan PDFeric parlNo ratings yet
- Immunity: Immunity Is The Balanced State ofDocument1 pageImmunity: Immunity Is The Balanced State ofCarolina GasperNo ratings yet
- Anatomy of LiverDocument22 pagesAnatomy of Liversiewv_1No ratings yet
- Palatine TonsilsDocument16 pagesPalatine TonsilsK.charitha ChowdaryNo ratings yet
- Stomach Peptic UlcerDocument38 pagesStomach Peptic UlcermohamedNo ratings yet
- Abdominal IncisionDocument4 pagesAbdominal IncisionMohit KumarNo ratings yet
- Adverse Drug EffectsDocument66 pagesAdverse Drug EffectsSuba Ranjana BalaNo ratings yet
- LRTIDocument13 pagesLRTIRomina Mae FajardoNo ratings yet
- Acute Inflammation: A Guide to the Protective ResponseDocument82 pagesAcute Inflammation: A Guide to the Protective ResponseBhanu PraseedhaNo ratings yet
- Effect of Acupressure On Physiological and Psychological Maladies Among Peri and Post Menopausal WomenDocument6 pagesEffect of Acupressure On Physiological and Psychological Maladies Among Peri and Post Menopausal WomenInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Anatomy and Physiology of The StomachDocument7 pagesAnatomy and Physiology of The StomachEmmi Maliza HutagaolNo ratings yet
- Arterial Blood PressureDocument46 pagesArterial Blood PressureRupasi KathiravanNo ratings yet
- Somatosensory Pathways: Primary Sensory and Motor AreasDocument36 pagesSomatosensory Pathways: Primary Sensory and Motor AreasAnonymous w3vYureNo ratings yet
- Presented By: VIVEK DEVDocument38 pagesPresented By: VIVEK DEVFranchesca LugoNo ratings yet
- Review of Anatomy and PhysiologyDocument7 pagesReview of Anatomy and PhysiologyKyla CalzadoNo ratings yet
- 04 - Soft Tissue InjuriesDocument13 pages04 - Soft Tissue InjuriesCielo GriñoNo ratings yet
- List of cranial nerves and their functionsDocument2 pagesList of cranial nerves and their functionsKay Lumpas Cruda100% (1)
- Human Skeleton-DlarsonDocument57 pagesHuman Skeleton-Dlarsonapi-308826929No ratings yet
- Cerebrovascular AccidentDocument30 pagesCerebrovascular AccidentJaydee Dalay100% (2)
- DISTRIBUTIVE SHOCKDocument41 pagesDISTRIBUTIVE SHOCKFuzi HannyNo ratings yet
- Increased Intracranial Pressure - StatPearls - NCBI BookshelfDocument5 pagesIncreased Intracranial Pressure - StatPearls - NCBI BookshelfWIWI HRNo ratings yet
- 10 - Anatomy of The Ear (Edited)Document26 pages10 - Anatomy of The Ear (Edited)Enlighten usNo ratings yet
- Classification & Clinical Features of LeprosyDocument41 pagesClassification & Clinical Features of LeprosyteslimolakunlerajiNo ratings yet
- Breast Pathology Fumc 2022Document145 pagesBreast Pathology Fumc 2022Bahzad AkramNo ratings yet
- Anatomy Exam Notes CNSPDFDocument60 pagesAnatomy Exam Notes CNSPDFBerk SonmezNo ratings yet
- Myasthenia Gravis: An Autoimmune Neurologic DisorderDocument16 pagesMyasthenia Gravis: An Autoimmune Neurologic DisorderHibba NasserNo ratings yet
- Miliary TB NewDocument23 pagesMiliary TB Newzakariah kamalNo ratings yet
- Gastrointestinal Anatomy and Physiology: The EssentialsFrom EverandGastrointestinal Anatomy and Physiology: The EssentialsJohn F. ReinusNo ratings yet
- Read MeDocument1 pageRead MeJauhar FirdausNo ratings yet
- ReleaseDocument1 pageReleaseGabriel StoicaNo ratings yet
- Installing InstructionsDocument1 pageInstalling InstructionsJauhar FirdausNo ratings yet
- Diabetes and KidneyDocument18 pagesDiabetes and KidneyJauhar FirdausNo ratings yet
- Pembuangan Sitrulin Pada Gagal GinjalDocument12 pagesPembuangan Sitrulin Pada Gagal GinjalJauhar FirdausNo ratings yet
- Fisiologi Olah RagaDocument37 pagesFisiologi Olah RagaJauhar Firdaus0% (1)
- AMR and and Rational Use of Antibiotics Workshop DR Mary Murray ReActDocument16 pagesAMR and and Rational Use of Antibiotics Workshop DR Mary Murray ReActJauhar FirdausNo ratings yet
- MTK device partition layout and settingsDocument6 pagesMTK device partition layout and settingsDrio RioNo ratings yet
- Generation of Gene-Modified Cynomolgus Monkey Via Cas9Document37 pagesGeneration of Gene-Modified Cynomolgus Monkey Via Cas9Jauhar FirdausNo ratings yet
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Monkey GeneDocument26 pagesMonkey GeneJauhar FirdausNo ratings yet
- Basic HIV AIDS PresentationDocument37 pagesBasic HIV AIDS PresentationRenny Marlina TorehNo ratings yet
- Testing Human Hair For Drugs of Abuse. IV. Environmental Cocaine Contamination and Washing EffectsDocument13 pagesTesting Human Hair For Drugs of Abuse. IV. Environmental Cocaine Contamination and Washing EffectsJauhar FirdausNo ratings yet
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Rational 2Document66 pagesRational 2Jauhar FirdausNo ratings yet
- RestoreUbuntu - XP - Vista - 7bootloader - Community Ubuntu DocumentationDocument4 pagesRestoreUbuntu - XP - Vista - 7bootloader - Community Ubuntu DocumentationJauhar FirdausNo ratings yet
- Physiology of PainDocument35 pagesPhysiology of PainJauhar Firdaus50% (2)
- ACOG Guideline For Perinatal CareDocument56 pagesACOG Guideline For Perinatal CareJauhar FirdausNo ratings yet
- Rational 2Document66 pagesRational 2Jauhar FirdausNo ratings yet
- ACOG Guideline For Perinatal CareDocument56 pagesACOG Guideline For Perinatal CareJauhar FirdausNo ratings yet
- Device For Detecting Methanol Concentration and The Method Thereof - Patent ApplicationDocument8 pagesDevice For Detecting Methanol Concentration and The Method Thereof - Patent ApplicationJauhar FirdausNo ratings yet
- Commen KontaminasiDocument1 pageCommen KontaminasiJauhar FirdausNo ratings yet
- Obesity Hypoventilation Syndrome (OHS) - MedlinePlus Medical EncyclopediaDocument3 pagesObesity Hypoventilation Syndrome (OHS) - MedlinePlus Medical EncyclopediaJauhar FirdausNo ratings yet
- Device For Detecting Methanol Concentration and The Method Thereof - Patent ApplicationDocument8 pagesDevice For Detecting Methanol Concentration and The Method Thereof - Patent ApplicationJauhar FirdausNo ratings yet
- Respon To Commen On MorphologicalDocument4 pagesRespon To Commen On MorphologicalJauhar FirdausNo ratings yet
- Morphine - Side Effects and Adverse ReactionsDocument2 pagesMorphine - Side Effects and Adverse ReactionsJauhar FirdausNo ratings yet
- Morphine PrecautionsDocument4 pagesMorphine PrecautionsJauhar FirdausNo ratings yet
- Morphine - Indications and DosageDocument4 pagesMorphine - Indications and DosageJauhar FirdausNo ratings yet
- Morphine - Chemisty and Biological ActivityDocument2 pagesMorphine - Chemisty and Biological ActivityJauhar FirdausNo ratings yet
- Appleton & Lange Review of Anatomy PDFDocument157 pagesAppleton & Lange Review of Anatomy PDFherry2sw100% (2)
- Chapter 14.1 - Cardiovascular System - Blood VesselsDocument56 pagesChapter 14.1 - Cardiovascular System - Blood VesselsMichael PeraltaNo ratings yet
- The Manchester Handbook of Ultrasound TechniquesDocument22 pagesThe Manchester Handbook of Ultrasound TechniquesAzie Azizah AGNo ratings yet
- Romanowky StainsDocument45 pagesRomanowky StainsFinu FarisaNo ratings yet
- Fertilization & ImplantationDocument61 pagesFertilization & ImplantationchidimmaNo ratings yet
- 1 Assessment: Subject: Scienceclass:2 Unit#1: The Human BodyDocument2 pages1 Assessment: Subject: Scienceclass:2 Unit#1: The Human BodyNatural Gas Metering Sui Norhern Gas Pipelines Ltd.No ratings yet
- Skin Functions and LayersDocument23 pagesSkin Functions and LayersAnis Samrotul Lathifah100% (2)
- Activacion de B Cells y Producción de Abs (2) CLASE RICHARD GARCIADocument49 pagesActivacion de B Cells y Producción de Abs (2) CLASE RICHARD GARCIAZuleynis MendozaNo ratings yet
- Unit 1 - Cell Structure and Organisation Without Slide Prep BackupDocument9 pagesUnit 1 - Cell Structure and Organisation Without Slide Prep BackupWaseem AhmedNo ratings yet
- 1 BAMS - MUHS Question PapersDocument45 pages1 BAMS - MUHS Question PapersShubham KaleNo ratings yet
- Chapter 21Document46 pagesChapter 21Quices AyingNo ratings yet
- Plant Reproduction: Asexual vs Sexual (39Document28 pagesPlant Reproduction: Asexual vs Sexual (39Lorine ChoiNo ratings yet
- Anatomy and Physiology of EarDocument15 pagesAnatomy and Physiology of EarShimmering MoonNo ratings yet
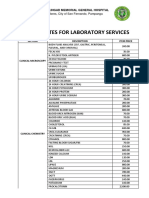
- JBLMGH Rates For Laboratory Services: Jose B. Lingad Memorial General HospitalDocument4 pagesJBLMGH Rates For Laboratory Services: Jose B. Lingad Memorial General HospitalApril NNo ratings yet
- BibliographyDocument9 pagesBibliographySam SamNo ratings yet
- 11.1 Antibody Production and VaccinationDocument28 pages11.1 Antibody Production and VaccinationFRENCHONLYNo ratings yet
- Diploma in KalariPayattu - Final Syllabus - 25 - 7 - 18Document18 pagesDiploma in KalariPayattu - Final Syllabus - 25 - 7 - 18Adhithya KiranNo ratings yet
- Skin Graft & FlapsDocument45 pagesSkin Graft & FlapsajNo ratings yet
- 2 BiomarkerDocument21 pages2 Biomarkerdiansutrisni95No ratings yet
- The Respiratory SystemDocument3 pagesThe Respiratory Systempaulo_camuaNo ratings yet
- CBC ReportDocument1 pageCBC ReportPranay BhosaleNo ratings yet
- Clinical Electrocardiography and ECG Interpretation - ECG & ECHODocument15 pagesClinical Electrocardiography and ECG Interpretation - ECG & ECHORimaNo ratings yet
- Science DLL Q2W1Document5 pagesScience DLL Q2W1ANGELBERT PEDNGANo ratings yet
- CH 11 Heart NotesDocument2 pagesCH 11 Heart Notesummnicole0% (1)
- Female Perineum and External Genitalia AnatomyDocument23 pagesFemale Perineum and External Genitalia AnatomySyed Irfan Arif100% (1)
- Comprehensive Elsevier Price List June 2012 Subject-WiseDocument47 pagesComprehensive Elsevier Price List June 2012 Subject-WiseMatin Ahmad KhanNo ratings yet
- Resolution of ABO Discrepancies: Justin R. Rhees, M.S., MLS (ASCP), SBBDocument41 pagesResolution of ABO Discrepancies: Justin R. Rhees, M.S., MLS (ASCP), SBBDumindu PereraNo ratings yet
- HematologyDocument5 pagesHematologyIvy Jan OcateNo ratings yet
- PRP RationaleDocument12 pagesPRP Rationalemarquezjayson548No ratings yet
- Vanishing Twin SacDocument14 pagesVanishing Twin SacAL MARIA MEDNo ratings yet