You might also like
- Knee Biomechanics: by Amrita..Document57 pagesKnee Biomechanics: by Amrita..Chanda NathaniNo ratings yet
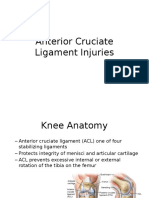
- Anterior Cruciate Ligament InjuriesDocument16 pagesAnterior Cruciate Ligament InjuriesAlmas PrawotoNo ratings yet
- Total Knee ReplacementDocument99 pagesTotal Knee ReplacementGandis Ayu WardaniNo ratings yet
- Floating Manipulative TherapyDocument7 pagesFloating Manipulative TherapyrahmatsahaquillaNo ratings yet
- Clinical Examination of Acute Adductor InjuriesDocument18 pagesClinical Examination of Acute Adductor Injuriessofianos100% (1)
- ShoulderDocument51 pagesShoulderIts LaraNo ratings yet
- Brachial Plexus ExaminationDocument7 pagesBrachial Plexus ExaminationMalvinder Singh DhillonNo ratings yet
- Exploring Cupping Today: A Beginners Course On Cupping Therapy & It's BenefitsFrom EverandExploring Cupping Today: A Beginners Course On Cupping Therapy & It's BenefitsNo ratings yet
- Soft Tissue Balance KneeDocument10 pagesSoft Tissue Balance KneeNitin BansalNo ratings yet
- A Patients Guide To Plantar Fasciitis Heel PainDocument4 pagesA Patients Guide To Plantar Fasciitis Heel PainJacobfranNo ratings yet
- 2 51 1656420123 1ijmpsdec20221Document4 pages2 51 1656420123 1ijmpsdec20221TJPRC PublicationsNo ratings yet
- Effect of Maitland Spinal Mobilization Therapy Versus Conventional Therapy in Lumbar Spondylosis With RadiculopathyDocument8 pagesEffect of Maitland Spinal Mobilization Therapy Versus Conventional Therapy in Lumbar Spondylosis With RadiculopathyjuancaNo ratings yet
- Weir Et Al. (2019) - Approaching Groin Pain in Athletics 'The Falcon's Perspective'Document8 pagesWeir Et Al. (2019) - Approaching Groin Pain in Athletics 'The Falcon's Perspective'Tom StevensNo ratings yet
- Carpal Tunnel SyndromeDocument2 pagesCarpal Tunnel Syndromeurkevet100% (1)
- What Is Shock Wave Therap 2Document7 pagesWhat Is Shock Wave Therap 2api-457017927No ratings yet
- Shoulder DislocationDocument6 pagesShoulder DislocationRizki IrwansyahNo ratings yet
- Soft Tissue Injuries of The KneeDocument3 pagesSoft Tissue Injuries of The KneeFarhan ShahidNo ratings yet
- Meniscus InjuryDocument29 pagesMeniscus InjurysolituNo ratings yet
- Assessment of KneeDocument113 pagesAssessment of KneeIqra Iftikhar100% (1)
- Pain and Motor Control 2011 HodgesDocument9 pagesPain and Motor Control 2011 HodgesPedro SilvaNo ratings yet
- Ombregt Ludwig. A System of Orthopaedic Medicine. 3th Edition. Elesvier. 2013. B9780702031458000867 - Web Pemeriksaan FisikDocument6 pagesOmbregt Ludwig. A System of Orthopaedic Medicine. 3th Edition. Elesvier. 2013. B9780702031458000867 - Web Pemeriksaan FisikSonia RogersNo ratings yet
- Application Technique Traction PDFDocument25 pagesApplication Technique Traction PDFAZOZ 19No ratings yet
- Pleural EffusionDocument78 pagesPleural EffusionJessa AdenigNo ratings yet
- PAE 5 Techniques of The Treatment With Faradic Type Current-1Document35 pagesPAE 5 Techniques of The Treatment With Faradic Type Current-1Huzaifa HabibNo ratings yet
- Journal Pre-Proof: ExploreDocument43 pagesJournal Pre-Proof: ExploreLuís CorreiaNo ratings yet
- Achilles TendonDocument30 pagesAchilles TendonMeldianaNo ratings yet
- Anatomy Trans UPPER EXTREMITIESDocument9 pagesAnatomy Trans UPPER EXTREMITIESSan LapuhapuNo ratings yet
- FES (Functional Electrical Stimulation)Document38 pagesFES (Functional Electrical Stimulation)Nivetha RavikumarNo ratings yet
- Pain and Pain Gate Control MechanismDocument17 pagesPain and Pain Gate Control MechanismKapil LakhwaraNo ratings yet
- Joint Mobilizations PDFDocument1 pageJoint Mobilizations PDFErik TellezNo ratings yet
- GL-PHYS-7 Total Knee ReplacementDocument8 pagesGL-PHYS-7 Total Knee Replacementandrei_costeaNo ratings yet
- Continuous Passive Motion Device BenefitsDocument9 pagesContinuous Passive Motion Device BenefitsAjay DherwaniNo ratings yet
- Tuberculosis of Hip JointDocument25 pagesTuberculosis of Hip JointYousra ShaikhNo ratings yet
- Introduction PhysiotherapistDocument12 pagesIntroduction Physiotherapistapi-371068989No ratings yet
- Specialtest Knee 140720123835 Phpapp01 PDFDocument146 pagesSpecialtest Knee 140720123835 Phpapp01 PDFlaszlo-368875100% (1)
- 香港脊醫 Hong Kong Chiropractors Sep 2016Document6 pages香港脊醫 Hong Kong Chiropractors Sep 2016CDAHKNo ratings yet
- Knee Injuries Part 1Document38 pagesKnee Injuries Part 1meenoNo ratings yet
- Distal Biceps Repair Rehabilitation Protocol by Tendayi MutsopotsiDocument5 pagesDistal Biceps Repair Rehabilitation Protocol by Tendayi MutsopotsiPhysiotherapy Care SpecialistsNo ratings yet
- Garv ResumeDocument5 pagesGarv Resumegarv_pt100% (1)
- Microwave DiathermyDocument19 pagesMicrowave DiathermyDale P. PolvorosaNo ratings yet
- Guidelines For Dry Needling Practice ISCP IrlandaDocument59 pagesGuidelines For Dry Needling Practice ISCP IrlandaDaniel VargasNo ratings yet
- Range of Motion Technique: by Anisa Altaf 18205 Presented To DR Sumeet Kumar Therapeutic ExcerciseDocument22 pagesRange of Motion Technique: by Anisa Altaf 18205 Presented To DR Sumeet Kumar Therapeutic ExcerciseArsal MushtaqNo ratings yet
- Theories of Pain MechanismDocument16 pagesTheories of Pain MechanismGithaiga KimaniNo ratings yet
- Meniscus Tears - Cartilage Damage: KneeDocument9 pagesMeniscus Tears - Cartilage Damage: KneedheenadayalanNo ratings yet
- Ankylosing Spondylitis Spine DiseaseDocument19 pagesAnkylosing Spondylitis Spine DiseaseZulhida YuniNo ratings yet
- Understanding and Managing Chronic Wounds: Jasmine Kartiko Pertiwi Jurusan Fisioterapi Poltekkes Kemenkes SurakartaDocument13 pagesUnderstanding and Managing Chronic Wounds: Jasmine Kartiko Pertiwi Jurusan Fisioterapi Poltekkes Kemenkes Surakartaamarilis sekarNo ratings yet
- MSK Low Back Pain Pathway Red Flag ScreeningDocument18 pagesMSK Low Back Pain Pathway Red Flag ScreeningMuhammed ElgasimNo ratings yet
- 2 Biomechanics of The ShoulderDocument47 pages2 Biomechanics of The ShoulderDaniel PereiraNo ratings yet
- Winback - en Brochure Rshock Version J3 Mars 2021 ADocument12 pagesWinback - en Brochure Rshock Version J3 Mars 2021 AThao Nguyen100% (1)
- ISMST GuidelinesDocument112 pagesISMST GuidelinesDhrubo TaraNo ratings yet
- Physiotherapy in Pakistan - An OverviewDocument4 pagesPhysiotherapy in Pakistan - An Overviewicrs_aamir100% (1)
- Introduction To Congestive Heart Failure Diagnosis, Classifications & ManagementDocument50 pagesIntroduction To Congestive Heart Failure Diagnosis, Classifications & Managementmadimadi11No ratings yet
- Frozen Shoulder JurnalDocument11 pagesFrozen Shoulder JurnalDandy DharmaNo ratings yet
- De Quervain S TenosynovitisDocument13 pagesDe Quervain S TenosynovitisPremaKurniaNo ratings yet
- Rotator Cuff Tears Orthoinfo - Aaos.org TopicDocument7 pagesRotator Cuff Tears Orthoinfo - Aaos.org TopicMontserrat LandaNo ratings yet
- Transcutaneous Electrical Nerve Stimulation (TENS)Document52 pagesTranscutaneous Electrical Nerve Stimulation (TENS)nobodyNo ratings yet
- Low Back PainDocument8 pagesLow Back PainLev KalikaNo ratings yet
- Antenatal and Postnatal PPT PDFDocument15 pagesAntenatal and Postnatal PPT PDFNikita -0251 ENo ratings yet
- Fawzia by Reda HarbyDocument111 pagesFawzia by Reda Harbyckyew64No ratings yet
- Prof - Amer Eltwati Ben Irhuma Consultant Surgeon Sebha Medical CollegeDocument79 pagesProf - Amer Eltwati Ben Irhuma Consultant Surgeon Sebha Medical Collegeckyew64100% (1)
- Ajdabya University Medical College - Colorectal Cancer Signs, Risks and ManagementDocument81 pagesAjdabya University Medical College - Colorectal Cancer Signs, Risks and Managementckyew64No ratings yet
- MRCS Clinical Examination Scheme & Test InterpretationDocument35 pagesMRCS Clinical Examination Scheme & Test Interpretationckyew64No ratings yet
- Peter Thiel’s CS183 Class 15 Notes on Energy Storage, Weather Prediction & Control, RoboticsDocument14 pagesPeter Thiel’s CS183 Class 15 Notes on Energy Storage, Weather Prediction & Control, Roboticsckyew64No ratings yet
- Manual For Renewing APCDocument15 pagesManual For Renewing APCJayagopi KadarasenNo ratings yet
- Colorectal Cancer: - Dr. Suneet KhuranaDocument36 pagesColorectal Cancer: - Dr. Suneet KhuranaCarlo ToledooNo ratings yet
- Anatomy LowerLimbAreasDocument4 pagesAnatomy LowerLimbAreasckyew64No ratings yet
- Surgeon's Gazettement LogbookDocument27 pagesSurgeon's Gazettement Logbookckyew64No ratings yet
- 2017 QR Management of Colorectal CarcinomaDocument8 pages2017 QR Management of Colorectal CarcinomaandrewNo ratings yet
- 11CPG-Non Variceal Upper Gastrointestinal BleedingDocument33 pages11CPG-Non Variceal Upper Gastrointestinal BleedingwitdechaNo ratings yet
- Peter Thiel's CS183: Startup - Class 18 Notes Essay: Joel CazaresDocument39 pagesPeter Thiel's CS183: Startup - Class 18 Notes Essay: Joel Cazaresckyew64No ratings yet
- Manage UA/NSTEMI Guideline 2011Document62 pagesManage UA/NSTEMI Guideline 2011Mohd RafiNo ratings yet
- Colorectal Cancer (CRC)Document43 pagesColorectal Cancer (CRC)ckyew64No ratings yet
- MOH Pocket Manual in General SurgeryDocument118 pagesMOH Pocket Manual in General SurgeryPavel LunaNo ratings yet
- Guide to Colorectal Carcinoma ManagementDocument99 pagesGuide to Colorectal Carcinoma Managementckyew64No ratings yet
- Asthma DrugsDocument2 pagesAsthma Drugsckyew64No ratings yet
- Peter Thiel's CS183Document13 pagesPeter Thiel's CS183ckyew64No ratings yet
- Peter Thiel 1Document6 pagesPeter Thiel 1Sreekanth PSNo ratings yet
- Anaphylaxis ManagementDocument9 pagesAnaphylaxis Managementckyew64No ratings yet
- Practice Guidelines For Central Venous Access PDFDocument35 pagesPractice Guidelines For Central Venous Access PDFJulio AltamiranoNo ratings yet
- Peter Thiel's CS183: Startup - Class 5 Notes EssayDocument7 pagesPeter Thiel's CS183: Startup - Class 5 Notes Essayckyew64No ratings yet
- Young and BeautifulDocument3 pagesYoung and Beautifulckyew64100% (1)
- Hip ExamDocument7 pagesHip Examckyew64No ratings yet
- Shoulder Exam Guide: Inspection, Palpation, ROM, Neurovascular, Special TestsDocument12 pagesShoulder Exam Guide: Inspection, Palpation, ROM, Neurovascular, Special Testsckyew64No ratings yet
- Case of The Week (Hypercalcemia)Document23 pagesCase of The Week (Hypercalcemia)ckyew64No ratings yet
- Hepatitis B StoryDocument8 pagesHepatitis B Storyckyew64No ratings yet
- M3 Park SensorDocument4 pagesM3 Park Sensorckyew64No ratings yet
- Letter To SS22A Residents 1way Traffic Flow - V2Document1 pageLetter To SS22A Residents 1way Traffic Flow - V2ckyew64No ratings yet
- Proposal For Funding of Computer Programme (NASS)Document6 pagesProposal For Funding of Computer Programme (NASS)Foster Boateng67% (3)
- Chapter 7 Project Cost ManagementDocument48 pagesChapter 7 Project Cost Managementafifah suyadiNo ratings yet
- Legend of GuavaDocument4 pagesLegend of GuavaRoem LeymaNo ratings yet
- ReportDocument7 pagesReportapi-482961632No ratings yet
- Unit 3 Activity 1-1597187907Document3 pagesUnit 3 Activity 1-1597187907Bryan SaltosNo ratings yet
- Placebo Studies Ritual TheoryDocument10 pagesPlacebo Studies Ritual Theoryapi-443830029No ratings yet
- Planning Levels and Types for Organizational SuccessDocument20 pagesPlanning Levels and Types for Organizational SuccessLala Ckee100% (1)
- 2009 IBP ElectionsDocument77 pages2009 IBP ElectionsBaldovino VenturesNo ratings yet
- Forum On Special Educational Needs: Phil Dexter Sharon Noseley Sophie FaragDocument14 pagesForum On Special Educational Needs: Phil Dexter Sharon Noseley Sophie Faragelena biancaNo ratings yet
- Jason A Brown: 1374 Cabin Creek Drive, Nicholson, GA 30565Document3 pagesJason A Brown: 1374 Cabin Creek Drive, Nicholson, GA 30565Jason BrownNo ratings yet
- TRU BRO 4pg-S120675R0 PDFDocument2 pagesTRU BRO 4pg-S120675R0 PDFtomNo ratings yet
- Operations Management Success FactorsDocument147 pagesOperations Management Success Factorsabishakekoul100% (1)
- Williams-In Excess of EpistemologyDocument19 pagesWilliams-In Excess of EpistemologyJesúsNo ratings yet
- Jaimini Astrology - Calculation of Mandook Dasha With A Case StudyDocument6 pagesJaimini Astrology - Calculation of Mandook Dasha With A Case StudyANTHONY WRITER100% (3)
- Touratsoglou, Coin Production and Circulation in Roman Peloponesus PDFDocument23 pagesTouratsoglou, Coin Production and Circulation in Roman Peloponesus PDFCromwellNo ratings yet
- Cronograma Ingles I v2Document1 pageCronograma Ingles I v2Ariana GarciaNo ratings yet
- Engineering: Ronnapee Chaichaowarat, Jun Kinugawa, Kazuhiro KosugeDocument8 pagesEngineering: Ronnapee Chaichaowarat, Jun Kinugawa, Kazuhiro Kosugelaura bemudezNo ratings yet
- International Journal of Current Advanced Research International Journal of Current Advanced ResearchDocument4 pagesInternational Journal of Current Advanced Research International Journal of Current Advanced Researchsoumya mahantiNo ratings yet
- p240 MemristorDocument5 pagesp240 MemristorGopi ChannagiriNo ratings yet
- FIRE Protection Engineering Winter 2002Document64 pagesFIRE Protection Engineering Winter 2002Hany RifaatNo ratings yet
- Hannah Money Resume 2Document2 pagesHannah Money Resume 2api-289276737No ratings yet
- 14 - Habeas Corpus PetitionDocument4 pages14 - Habeas Corpus PetitionJalaj AgarwalNo ratings yet
- Essay A Level Drama and Theatee Studies A LevelDocument2 pagesEssay A Level Drama and Theatee Studies A LevelSofia NietoNo ratings yet
- Photojournale - Connections Across A Human PlanetDocument75 pagesPhotojournale - Connections Across A Human PlanetjohnhorniblowNo ratings yet
- 02 Cost of Capital QBDocument26 pages02 Cost of Capital QBAbhi JayakumarNo ratings yet
- Audience AnalysisDocument7 pagesAudience AnalysisSHAHKOT GRIDNo ratings yet
- Analyzing Evidence of College Readiness: A Tri-Level Empirical & Conceptual FrameworkDocument66 pagesAnalyzing Evidence of College Readiness: A Tri-Level Empirical & Conceptual FrameworkJinky RegonayNo ratings yet
- 1000 Electronic Devices & Circuits MCQsDocument467 pages1000 Electronic Devices & Circuits MCQskibrom atsbha67% (3)
- Course Syllabus (NGCM 112)Document29 pagesCourse Syllabus (NGCM 112)Marie Ashley Casia100% (1)