You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Emergency Department TriageDocument139 pagesEmergency Department TriageEddy Liem100% (2)
- Hematemesis Melena (Upper Gi Bleeding)Document134 pagesHematemesis Melena (Upper Gi Bleeding)Mardoni Efrijon100% (1)
- Problem PrioritizationDocument2 pagesProblem PrioritizationFlauros Ryu Jabien100% (3)
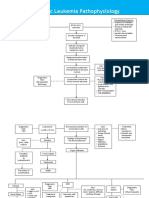
- Acute Lymphoblastic Leukemia Pathophysiology: Predisposing Factors: Etiology: Precipitating FactorsDocument3 pagesAcute Lymphoblastic Leukemia Pathophysiology: Predisposing Factors: Etiology: Precipitating FactorsKyla ValenciaNo ratings yet
- Trypanosomiasis & LeishmaniasisDocument50 pagesTrypanosomiasis & LeishmaniasisMardoni Efrijon75% (4)
- Group 4 Case Study On Malignant MelanomaDocument7 pagesGroup 4 Case Study On Malignant MelanomaLance JardiolinNo ratings yet
- DMDocument106 pagesDMMardoni Efrijon100% (1)
- TaeniasisDocument23 pagesTaeniasisMardoni Efrijon33% (3)
- Evaluation of The Gene Xpert For Human Monkeypox Diagnosis: Zahra Inayah Kasim, Nursin Abd - Kadir, Benny RusliDocument15 pagesEvaluation of The Gene Xpert For Human Monkeypox Diagnosis: Zahra Inayah Kasim, Nursin Abd - Kadir, Benny Ruslizahra inayahNo ratings yet
- Manual: Federal Ministry of Health EthiopiaDocument196 pagesManual: Federal Ministry of Health Ethiopiaalfonso delgadoNo ratings yet
- Glaukoma: Dr. Mandiri Nindiasari, SPM, MSCDocument59 pagesGlaukoma: Dr. Mandiri Nindiasari, SPM, MSCfebienaNo ratings yet
- Quality Assurance RSDocument17 pagesQuality Assurance RSMardoni EfrijonNo ratings yet
- Pelayanan Kesehatan Primer Di Rumah Sakit Dan PuskesmasDocument14 pagesPelayanan Kesehatan Primer Di Rumah Sakit Dan PuskesmasMardoni EfrijonNo ratings yet
- Hypoglicemia-Endocrin 3Document54 pagesHypoglicemia-Endocrin 3Ihsan AndanNo ratings yet
- TonsilofaringitisDocument23 pagesTonsilofaringitisMardoni EfrijonNo ratings yet
- Sistem Respirasi UnibaDocument86 pagesSistem Respirasi UnibaMardoni EfrijonNo ratings yet
- Rinitis Alergi Dan VasomotorDocument26 pagesRinitis Alergi Dan VasomotorMardoni EfrijonNo ratings yet
- CARDIOLOGY DecompensatioDocument168 pagesCARDIOLOGY Decompensatioyurie_ameliaNo ratings yet
- TonsilofaringitisDocument23 pagesTonsilofaringitisMardoni EfrijonNo ratings yet
- Sistem Respirasi UnibaDocument86 pagesSistem Respirasi UnibaMardoni EfrijonNo ratings yet
- ToxoplasmosisDocument28 pagesToxoplasmosisMardoni EfrijonNo ratings yet
- Sistem Respirasi UnibaDocument86 pagesSistem Respirasi UnibaMardoni EfrijonNo ratings yet
- Gangguan Siklus MenstruasiDocument26 pagesGangguan Siklus MenstruasiMardoni EfrijonNo ratings yet
- Malaria KlinisDocument44 pagesMalaria KlinisMardoni EfrijonNo ratings yet
- Malaria KlinisDocument44 pagesMalaria KlinisMardoni EfrijonNo ratings yet
- Schistosomiasis & FascioliosisDocument40 pagesSchistosomiasis & FascioliosisWahyudi YusmanNo ratings yet
- Intestinal Protozoa: Parasitology DeptDocument21 pagesIntestinal Protozoa: Parasitology DeptWahyudi YusmanNo ratings yet
- JURNAL2Document14 pagesJURNAL2Mardoni EfrijonNo ratings yet
- Filaria 2012 - RevDocument34 pagesFilaria 2012 - RevMardoni EfrijonNo ratings yet
- Intestinal Protozoa: Parasitology DeptDocument21 pagesIntestinal Protozoa: Parasitology DeptWahyudi YusmanNo ratings yet
- Rheumatoid ArthritisDocument66 pagesRheumatoid ArthritisSaeda AhmedNo ratings yet
- Parasitology Definitions and Host TypesDocument2 pagesParasitology Definitions and Host TypesIzy GomezNo ratings yet
- 2 - EBM PrognosisDocument44 pages2 - EBM PrognosisWahyu adi PratamaNo ratings yet
- Sop Alur Pelayanan Pasien TB Rawat JalandocDocument336 pagesSop Alur Pelayanan Pasien TB Rawat JalandocRahayu HidayatiNo ratings yet
- Presentation On Incidence and PrevalenceDocument17 pagesPresentation On Incidence and PrevalenceSUBHNo ratings yet
- Carlos - Gualpa - Individual Work PDFDocument2 pagesCarlos - Gualpa - Individual Work PDFCarlos GualpaNo ratings yet
- Hypochondriasis and PainDocument4 pagesHypochondriasis and PainAparajitaNo ratings yet
- A Clinicohematological Profile of SplenomegalyDocument6 pagesA Clinicohematological Profile of SplenomegalyIvan Louis ToledoNo ratings yet
- Catedra Ramazzini. Desafios y Oportunidades de La Salud Ocupacional Dr. Yukka Takala PDFDocument41 pagesCatedra Ramazzini. Desafios y Oportunidades de La Salud Ocupacional Dr. Yukka Takala PDFArledis Acevedo GonzálezNo ratings yet
- Temperoray Internal Jugular Catheter (Ijc) For Chronic Hemodialysis PatientsDocument2 pagesTemperoray Internal Jugular Catheter (Ijc) For Chronic Hemodialysis PatientsBobby Chin SinghNo ratings yet
- Antibiotics For CssDocument38 pagesAntibiotics For CsstayyabsaifNo ratings yet
- QUESTIONAIRE Research Final PDFDocument2 pagesQUESTIONAIRE Research Final PDFAli AfaqNo ratings yet
- Dengue: What Is Dengue Fever? What Is Dengue Hemorrhagic Fever?Document9 pagesDengue: What Is Dengue Fever? What Is Dengue Hemorrhagic Fever?Abdul Shakur FaisalNo ratings yet
- Case Analysis 3.0Document3 pagesCase Analysis 3.0Shane Fross SeñedoNo ratings yet
- Cohort Study - Study Design 101Document2 pagesCohort Study - Study Design 101Sahil sharmaNo ratings yet
- BGS ISBT Antigens Antibodies and Associated DiseasesDocument1 pageBGS ISBT Antigens Antibodies and Associated DiseasesIya BangalanNo ratings yet
- CDC guidelines for treating syphilisDocument27 pagesCDC guidelines for treating syphilisGabrielaGushikenNo ratings yet
- TOXOPLASMOSIS: Diagnosis, Treatment and Prevention in Congenitally Exposed InfantsDocument30 pagesTOXOPLASMOSIS: Diagnosis, Treatment and Prevention in Congenitally Exposed InfantshwelpNo ratings yet
- Brain Tumor New 1Document6 pagesBrain Tumor New 1Tiiffanyy Faiith PadillaNo ratings yet
- SCRIPT For MTAPDocument3 pagesSCRIPT For MTAPGia UrdaiaNo ratings yet
- BURKHOLDERIADocument6 pagesBURKHOLDERIAFatima AbasovaNo ratings yet
- Lesson Plan in English Transcode Linear To Non Linear and Vice VersaDocument5 pagesLesson Plan in English Transcode Linear To Non Linear and Vice VersaRoneca BatucanNo ratings yet
- 2016 European Guideline on Management of Epididymo-OrchitisDocument6 pages2016 European Guideline on Management of Epididymo-OrchitisdidiNo ratings yet
- 47-Article Text-305-1-10-20220731Document10 pages47-Article Text-305-1-10-20220731alyn30274No ratings yet
- Reseach ProposalDocument8 pagesReseach Proposaljoyce marie asucanNo ratings yet