You might also like
- Pediatric Hematology: Division of Hematology & Oncology Child Health DepartmentDocument37 pagesPediatric Hematology: Division of Hematology & Oncology Child Health DepartmentIsmail Satrio WibowoNo ratings yet
- Hematology& Onco LectureDocument66 pagesHematology& Onco Lecturehasanatiya41No ratings yet
- Hematological DisordersDocument45 pagesHematological Disordersbara.jarrar2001No ratings yet
- Blood Disorders Seminar No 7Document142 pagesBlood Disorders Seminar No 7Hysum Mushtaq100% (1)
- Hematology Oncology Nplex ReviewDocument46 pagesHematology Oncology Nplex ReviewValeria AcevedoNo ratings yet
- BloodDocument142 pagesBloodChelleyOllitroNo ratings yet
- Causes and Treatment of Anemia in ChildrenDocument33 pagesCauses and Treatment of Anemia in ChildrenYemata HailuNo ratings yet
- Hemolytic AnemiasDocument59 pagesHemolytic AnemiasRajesh darlingNo ratings yet
- Blood Basics1Document6 pagesBlood Basics1Celina PastorNo ratings yet
- RBC DISORDERS StudentsDocument84 pagesRBC DISORDERS Studentskimberly abianNo ratings yet
- Anemia Is A Laboratory Diagnosis: Men WomenDocument21 pagesAnemia Is A Laboratory Diagnosis: Men WomenOmaraye JoshuaNo ratings yet
- Anemia SDocument125 pagesAnemia SamirhsheikhiNo ratings yet
- Essential facts about anemia in pregnancyDocument40 pagesEssential facts about anemia in pregnancyraph faith100% (1)
- Disampaikan Oleh: Dr. Ong Tjandra, MMPD., Spog (K)Document46 pagesDisampaikan Oleh: Dr. Ong Tjandra, MMPD., Spog (K)Asis muhammadNo ratings yet
- Microcytic Normocytic and Macrocytic: by DR Hodan Jama 02/12/2017Document47 pagesMicrocytic Normocytic and Macrocytic: by DR Hodan Jama 02/12/2017Abdisalan hassanNo ratings yet
- Anemia in Infancy: Causes, Diagnosis and ManagementDocument40 pagesAnemia in Infancy: Causes, Diagnosis and ManagementSachitra RathodNo ratings yet
- AnemiaDocument41 pagesAnemiaBang FadNo ratings yet
- Anemia Anak 2: Dr. BerthaDocument35 pagesAnemia Anak 2: Dr. BerthaAriNo ratings yet
- Hematologic DisorderDocument16 pagesHematologic DisorderZoe DorothyNo ratings yet
- Thalassaemia - : Dr. KAW KarunasekeraDocument36 pagesThalassaemia - : Dr. KAW KarunasekerarikarzNo ratings yet
- Approach To Anemia: Bisrat DDocument45 pagesApproach To Anemia: Bisrat Dyared getachewNo ratings yet
- Dr. THOMAS KINGSLEY MD Professor of Medicine TVMCDocument48 pagesDr. THOMAS KINGSLEY MD Professor of Medicine TVMCDr THOMAS KINGSLEY MDNo ratings yet
- Abnormal HBDocument55 pagesAbnormal HBtofyNo ratings yet
- Hematology summary guideDocument91 pagesHematology summary guidePeter Shirima100% (1)
- Haematological DisordersDocument28 pagesHaematological DisordersSamuel kuriaNo ratings yet
- ThalassemiaDocument14 pagesThalassemiaDeepthi AvvaruNo ratings yet
- Basic Lab InvestigationsDocument121 pagesBasic Lab InvestigationsTheop Ayodele100% (1)
- Pediatric Hematology LectureDocument84 pagesPediatric Hematology LectureloitaNo ratings yet
- BloodDocument80 pagesBloodHem Chandra ShahNo ratings yet
- Eac HemaDocument150 pagesEac HemaRemelou Garchitorena AlfelorNo ratings yet
- Anemia in ChildrenDocument67 pagesAnemia in ChildrenAgung Maulana ArmstrongNo ratings yet
- Blood Transfusion Blood Grouping and Cross MatchingDocument46 pagesBlood Transfusion Blood Grouping and Cross MatchingHa LeemNo ratings yet
- Thalassemia-Engleza NouDocument73 pagesThalassemia-Engleza NouDM XyzNo ratings yet
- Anemia-Dr Moses KazevuDocument86 pagesAnemia-Dr Moses KazevuMoses Jr KazevuNo ratings yet
- Thalassemia SyndromesDocument29 pagesThalassemia SyndromesIsaac MwangiNo ratings yet
- Bloodkb 160720181259Document129 pagesBloodkb 160720181259Jeena RajNo ratings yet
- Leukamia and Transfusion MedicineDocument26 pagesLeukamia and Transfusion MedicineSamuel kuriaNo ratings yet
- Neonatal AnemiaDocument22 pagesNeonatal AnemiaFebrina Utami Putri100% (4)
- Anemia in ChildrenDocument67 pagesAnemia in ChildrenDenny BimatamaNo ratings yet
- Red Blood Cells and Anemias: Jonathan Ben-Ezra, M.DDocument33 pagesRed Blood Cells and Anemias: Jonathan Ben-Ezra, M.Diloveit52252No ratings yet
- Sickle Cell AnemiaDocument42 pagesSickle Cell Anemiaaafrah100% (2)
- Chapter 44: Nursing Care of The Client With An Hematologic DisordersDocument18 pagesChapter 44: Nursing Care of The Client With An Hematologic DisordersfLOR_ZIANE_MAENo ratings yet
- Blood Transfusion JottingsDocument49 pagesBlood Transfusion JottingsAishat AwodeleNo ratings yet
- Anemia in PregnancyDocument18 pagesAnemia in Pregnancysaagiba100% (1)
- Anemia in Childhood, Physiopathology and Clinical Findings Bleeding Tests in ChildhoodDocument76 pagesAnemia in Childhood, Physiopathology and Clinical Findings Bleeding Tests in Childhoodmohammed barwaryNo ratings yet
- Approach To AnemiaDocument50 pagesApproach To AnemiaRishi ShresthaNo ratings yet
- Hematologic DxsDocument34 pagesHematologic DxsAYTONA, JAMAICA F.No ratings yet
- New Psychiatry FAE2016Document120 pagesNew Psychiatry FAE2016omarNo ratings yet
- AnemiaDocument63 pagesAnemiaRasoulNo ratings yet
- Anemia NotesDocument6 pagesAnemia NotesElstella Eguavoen Ehicheoya100% (2)
- Anemia Classification and Assesment: Kebirungi Caroline BMS/0077/133/DUDocument35 pagesAnemia Classification and Assesment: Kebirungi Caroline BMS/0077/133/DUkivumbi AchileoNo ratings yet
- Thalassemia 200510173444Document31 pagesThalassemia 200510173444sharifiNo ratings yet
- انيماDocument59 pagesانيمااحمد احمدNo ratings yet
- Lecture 4 - Hematology-PedsDocument60 pagesLecture 4 - Hematology-PedsGelsey Gelsinator JianNo ratings yet
- Hematological DisorderDocument49 pagesHematological DisorderSandeepNo ratings yet
- Major Functions of the Circulatory SystemDocument26 pagesMajor Functions of the Circulatory SystemDrSikander AdilNo ratings yet
- Anaemias Guide: Causes, Symptoms and TreatmentDocument41 pagesAnaemias Guide: Causes, Symptoms and Treatmentbrian mgabiNo ratings yet
- _تفسیر آزمایشات روتینDocument116 pages_تفسیر آزمایشات روتینrajabisamira8No ratings yet
- Fast Facts: Deficit di piruvato chinasi per pazienti e sostenitori: Una rara malattia genetica che colpisce I globuli rossi Informazioni + assunzione del controllo = migliore risultatoFrom EverandFast Facts: Deficit di piruvato chinasi per pazienti e sostenitori: Una rara malattia genetica che colpisce I globuli rossi Informazioni + assunzione del controllo = migliore risultatoNo ratings yet
- The Many Presentations of Inherited Metabolic DiseasesDocument31 pagesThe Many Presentations of Inherited Metabolic DiseasesMateen ShukriNo ratings yet
- Best Evidence Medical EducationDocument24 pagesBest Evidence Medical EducationMateen ShukriNo ratings yet
- MasDocument41 pagesMasMateen ShukriNo ratings yet
- Hemostasis 19-3-2012Document11 pagesHemostasis 19-3-2012Mateen ShukriNo ratings yet
- Rectus Sheath Catheters in Children Clinical Guideline For UseDocument8 pagesRectus Sheath Catheters in Children Clinical Guideline For UseMateen ShukriNo ratings yet
- PAEDIATRICS Notes 3 Update PDFDocument69 pagesPAEDIATRICS Notes 3 Update PDFMateen ShukriNo ratings yet
- MRCPCH2 Exam 17.9.2014Document14 pagesMRCPCH2 Exam 17.9.2014Mateen ShukriNo ratings yet
- GuidelinesDocument253 pagesGuidelinesDestia AnandaNo ratings yet
- Evidence Informed Professional Education Practice and PolicyDocument22 pagesEvidence Informed Professional Education Practice and PolicyMateen ShukriNo ratings yet
- Definition of Genetic CounsellingDocument6 pagesDefinition of Genetic CounsellingMateen ShukriNo ratings yet
- Git 2Document18 pagesGit 2Mateen ShukriNo ratings yet
- Resmanual PDFDocument41 pagesResmanual PDFMateen ShukriNo ratings yet
- Categorized List of BehaviorsDocument4 pagesCategorized List of BehaviorsMateen ShukriNo ratings yet
- Fluid & Electrolyte MetabolismDocument12 pagesFluid & Electrolyte MetabolismMateen ShukriNo ratings yet
- Tuberculosis: An Approach To A Child WithDocument25 pagesTuberculosis: An Approach To A Child WithMateen ShukriNo ratings yet
- Pediatric Q&ADocument12 pagesPediatric Q&AMateen ShukriNo ratings yet
- Pediatric Toxicology: Nga B. Pham, M.DDocument90 pagesPediatric Toxicology: Nga B. Pham, M.DMateen ShukriNo ratings yet
- Inflammatory Joint Diseases Reference GuideDocument13 pagesInflammatory Joint Diseases Reference GuideMateen ShukriNo ratings yet
- Fluids&LytesDocument33 pagesFluids&LytesMateen ShukriNo ratings yet
- Common issues in neonatal careDocument41 pagesCommon issues in neonatal careIrwan MuhaiminNo ratings yet
- 18Document30 pages18Mateen ShukriNo ratings yet
- Altered Mental StatusDocument19 pagesAltered Mental StatusMateen ShukriNo ratings yet
- Understanding Hyperbilirubinemia in NewbornsDocument33 pagesUnderstanding Hyperbilirubinemia in NewbornsMateen ShukriNo ratings yet
- Answer of Infection and Immunology Mock Exam 9Document7 pagesAnswer of Infection and Immunology Mock Exam 9Mateen ShukriNo ratings yet
- Clinical Quiz: What Is The Diagnosis?Document1 pageClinical Quiz: What Is The Diagnosis?Mateen ShukriNo ratings yet
- Malnutrition Vitamins and MineralsDocument1 pageMalnutrition Vitamins and MineralsMateen ShukriNo ratings yet
- Antibiotic Recommendations WC 2012Document67 pagesAntibiotic Recommendations WC 2012Mateen ShukriNo ratings yet
- Icc Uptodate PDFDocument17 pagesIcc Uptodate PDFclaudia franciaNo ratings yet
- Emergency Pediatric Imaging Quiz Case 1: Continuing Medical Education Áãüôåøõþûôüöøñâàøùöôùßñø ÔãáöDocument2 pagesEmergency Pediatric Imaging Quiz Case 1: Continuing Medical Education Áãüôåøõþûôüöøñâàøùöôùßñø ÔãáöMateen ShukriNo ratings yet
- Other Blood Group SystemDocument42 pagesOther Blood Group SystemCarla May Orange GualbertoNo ratings yet
- Erythroblastosis Fetalis - Gynecology and Obstetrics - MSD Manual Professional EditionDocument3 pagesErythroblastosis Fetalis - Gynecology and Obstetrics - MSD Manual Professional EditionNike KomalaNo ratings yet
- The Internet Journal of Gynecology and ObstetricsDocument8 pagesThe Internet Journal of Gynecology and Obstetricsrett_ttaNo ratings yet
- Polansky SKRRT PDFDocument619 pagesPolansky SKRRT PDFAstrud Labrador100% (1)
- Chap 6-7 Modern Blood Banking & Transfusion Practices (PDFDrive) (1) - Pages-138-190Document53 pagesChap 6-7 Modern Blood Banking & Transfusion Practices (PDFDrive) (1) - Pages-138-190Patricia Marie de OcampoNo ratings yet
- Blood WorksheetDocument2 pagesBlood WorksheetNadia ShafiqNo ratings yet
- HaematologyDocument68 pagesHaematologytapoolnoNo ratings yet
- Amniotic Fluid AnalysisDocument6 pagesAmniotic Fluid Analysisdan paolo sanchezNo ratings yet
- A Compendium of Tranfusion Prectice Guidelines ARC Edition 4.0 Jan 2021Document75 pagesA Compendium of Tranfusion Prectice Guidelines ARC Edition 4.0 Jan 2021H Stuard B CocNo ratings yet
- University of Gondar College of Medicine and Health ScienceDocument100 pagesUniversity of Gondar College of Medicine and Health ScienceCHALIE MEQUNo ratings yet
- OBSTETRICSDocument4 pagesOBSTETRICSjamie carpioNo ratings yet
- Assignment: Department of PhysiologyDocument34 pagesAssignment: Department of PhysiologyMaria NeyveliNo ratings yet
- Human Health & DiseasesDocument55 pagesHuman Health & DiseasesSAGAR PADALKARNo ratings yet
- Iso ImmunizationDocument3 pagesIso ImmunizationHazel Marie EchavezNo ratings yet
- RH Incompatibility: Swatilekha Das (RN, MSN)Document15 pagesRH Incompatibility: Swatilekha Das (RN, MSN)jyoti kundu100% (1)
- Lynetteskie: Larger Than Erythrocytes Function: Fight Infections & Remove Dead Cells & DebrisDocument4 pagesLynetteskie: Larger Than Erythrocytes Function: Fight Infections & Remove Dead Cells & DebrisCamilleCalmaLenonNo ratings yet
- Allergy BDS Seminar ReportDocument21 pagesAllergy BDS Seminar ReportErSandeepVermaNo ratings yet
- Blood Groups, Abo and RHDocument6 pagesBlood Groups, Abo and RHromeoenny4154No ratings yet
- Blood (Anaphy)Document8 pagesBlood (Anaphy)CORONEL, SOPHIANo ratings yet
- Health Education On NEONATAL JAUNDICEDocument23 pagesHealth Education On NEONATAL JAUNDICEAsha jilu100% (2)
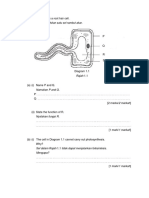
- Root hair cell structure and functionsDocument29 pagesRoot hair cell structure and functionsAzfar SyahmiNo ratings yet
- Hypertension in PregnancyDocument8 pagesHypertension in PregnancyHannrhey VelascoNo ratings yet
- BiliDocument63 pagesBiliFu Xiao ShanNo ratings yet
- HypersensitivityDocument20 pagesHypersensitivityJAIRA RIEYELLE LIPANANo ratings yet
- Drury, Hill, Chitty - 2016 - Cell-Free Fetal DNA Testing For Prenatal DiagnosisDocument35 pagesDrury, Hill, Chitty - 2016 - Cell-Free Fetal DNA Testing For Prenatal DiagnosisCindy KestyNo ratings yet
- IMHM321 Lecture Trans 3Document9 pagesIMHM321 Lecture Trans 3Brix BrixNo ratings yet
- KMLTTB May 2015 Theory Papers-1-2Document31 pagesKMLTTB May 2015 Theory Papers-1-2ephantusNo ratings yet
- Blood Banking Progress ExamDocument67 pagesBlood Banking Progress ExamlenvycahpdelusaNo ratings yet
- Heme Synthesis Breakdown HBDocument18 pagesHeme Synthesis Breakdown HBDr.P.NatarajanNo ratings yet
- Pediatric S: The Journal ofDocument9 pagesPediatric S: The Journal ofFandi ArgiansyaNo ratings yet