You might also like
- Fondaparinux in Acute Coronary Syndromes CA5068 Admin OnlyDocument9 pagesFondaparinux in Acute Coronary Syndromes CA5068 Admin OnlynaeamzNo ratings yet
- Fondaparinux - Grand - Rounds ACSDocument29 pagesFondaparinux - Grand - Rounds ACSSurya MahardikaNo ratings yet
- Perioperative Anesthesia Anagement OnDocument30 pagesPerioperative Anesthesia Anagement OnryandikaNo ratings yet
- From Efficacy and Safety of Fondaparinux in Management of ACSDocument35 pagesFrom Efficacy and Safety of Fondaparinux in Management of ACSNur Cahyani SetiawatiNo ratings yet
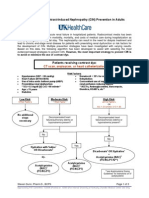
- Contrast NephRopathy GuidelinesDocument3 pagesContrast NephRopathy GuidelinesStacey WoodsNo ratings yet
- White 2012 Champion PooledDocument13 pagesWhite 2012 Champion PooledRadu CiprianNo ratings yet
- MIMS Doctor August 2016 RGDocument43 pagesMIMS Doctor August 2016 RGDeddy SupriyadiNo ratings yet
- PolipillDocument10 pagesPolipillSMIBA MedicinaNo ratings yet
- SUP in ICU SlidesDocument36 pagesSUP in ICU SlidesAgus SyaifudinNo ratings yet
- ACC/AHA STEMI GuidelinesDocument94 pagesACC/AHA STEMI GuidelinesDika DekokNo ratings yet
- Sun002 PDFDocument8 pagesSun002 PDFmmmaw mmNo ratings yet
- Evidencia Clinica de Antiagregantes Plaquetarios y Ima 2015Document11 pagesEvidencia Clinica de Antiagregantes Plaquetarios y Ima 2015Edgar PazNo ratings yet
- ARTICLEDocument13 pagesARTICLEHamzah MohiuddinNo ratings yet
- Guidelines of Implementation For The Management of Acs Focus On Coronary InterventionDocument33 pagesGuidelines of Implementation For The Management of Acs Focus On Coronary InterventionannisNo ratings yet
- Iacta 2011 Janak Mehta Award Winning PresentationDocument56 pagesIacta 2011 Janak Mehta Award Winning PresentationDr.Sandeep Kumar KarNo ratings yet
- Cost-Effectiveness of Fondaparinux Versus Enoxaparin in non-ST-elevation Acute Coronary Syndrome in Canada (OASIS-5)Document6 pagesCost-Effectiveness of Fondaparinux Versus Enoxaparin in non-ST-elevation Acute Coronary Syndrome in Canada (OASIS-5)Eko Persia NurhidayatNo ratings yet
- Treatment Approach Considerations: Pericardial SclerosisDocument7 pagesTreatment Approach Considerations: Pericardial SclerosisDikie MustofadijayaNo ratings yet
- COPPSDocument6 pagesCOPPSleoquerNo ratings yet
- Pengunaan Ubat-Islam - Kes Scenario (Prof Wan Azman PPUM)Document21 pagesPengunaan Ubat-Islam - Kes Scenario (Prof Wan Azman PPUM)bebytycoNo ratings yet
- Aas - Hasta IqDocument8 pagesAas - Hasta IqFrancisco A. Perez JimenezNo ratings yet
- Ultra-Early Tranexamic Acid After Subarachnoid Hemorrhage (ULTRA) : Study Protocol For A Randomized Controlled TrialDocument7 pagesUltra-Early Tranexamic Acid After Subarachnoid Hemorrhage (ULTRA) : Study Protocol For A Randomized Controlled Trialrikadwi20No ratings yet
- TOPIC 01 - Coronary Heart Disease: January 13, Thursday 2011Document1 pageTOPIC 01 - Coronary Heart Disease: January 13, Thursday 2011pppijkNo ratings yet
- Pi Is 0007091217540015Document10 pagesPi Is 0007091217540015Yoga WibowoNo ratings yet
- Dream Trial Journal PresentationDocument30 pagesDream Trial Journal PresentationRam Kumar ShresthaNo ratings yet
- Angina 22Document3 pagesAngina 22Aqa Mirza Muhammad Al-SyahabadiNo ratings yet
- EsomeprazoleDocument7 pagesEsomeprazoleSanjay NavaleNo ratings yet
- Significant Early In-Hospital Benefit Was Seen. Clopidogrel Is Prefferd ToDocument8 pagesSignificant Early In-Hospital Benefit Was Seen. Clopidogrel Is Prefferd TogilnifNo ratings yet
- Clopidogrel: 26% More Effective than AspirinDocument30 pagesClopidogrel: 26% More Effective than AspirinMuhammad Yolandi SumadioNo ratings yet
- Haemorrhage and Risk Factors Associated With RetrobulbarDocument12 pagesHaemorrhage and Risk Factors Associated With RetrobulbarVidola Yasena PutriNo ratings yet
- MICHELLE Trial - Rivaroxaban Versus No Anticoagulation ForDocument18 pagesMICHELLE Trial - Rivaroxaban Versus No Anticoagulation ForSheerazNo ratings yet
- 50000520210101Document7 pages50000520210101Amaliah HakimNo ratings yet
- Platelet Glycoprotein Iib/Iiia Inhibition With Coronary Stenting For Acute Myocardial InfarctionDocument9 pagesPlatelet Glycoprotein Iib/Iiia Inhibition With Coronary Stenting For Acute Myocardial InfarctionJanuar RezkyNo ratings yet
- ESCAPE Study - JAMA 2005Document9 pagesESCAPE Study - JAMA 2005MICHAEL AMARILLO CORREANo ratings yet
- Clinical AuditDocument4 pagesClinical Audithims.qualitymanagerNo ratings yet
- Evidence Based Stroke Medicine. Evaluating Treatments For Acute Ischaemic Stroke - What Works and What Doesn't?Document32 pagesEvidence Based Stroke Medicine. Evaluating Treatments For Acute Ischaemic Stroke - What Works and What Doesn't?maluku barat dayaNo ratings yet
- Ischemic 19Document8 pagesIschemic 19Adina Alexandra CNo ratings yet
- Steroids in Cardiac SurgeryDocument52 pagesSteroids in Cardiac SurgeryKarthik RamanNo ratings yet
- Percutaneous Cardiac Support During Myocardial Infarction Drastically Reduces Mortality: Perspectives From A Swine ModelDocument7 pagesPercutaneous Cardiac Support During Myocardial Infarction Drastically Reduces Mortality: Perspectives From A Swine ModelAdrian BratuNo ratings yet
- Updates From The New American College of Chest Physicians: Antithrombotic Therapy and Prevention of Thrombosis, 9 EditionDocument22 pagesUpdates From The New American College of Chest Physicians: Antithrombotic Therapy and Prevention of Thrombosis, 9 Editionbuddho81No ratings yet
- Surgery Oral Sildenafil To Control Pulmonary Hypertension After Congenital HeartDocument7 pagesSurgery Oral Sildenafil To Control Pulmonary Hypertension After Congenital HeartYuliawati GayoNo ratings yet
- Acute Myocardial Infarction: Primary Angioplasty: Coronary DiseaseDocument5 pagesAcute Myocardial Infarction: Primary Angioplasty: Coronary DiseaseGuțu SergheiNo ratings yet
- Atrial Flutter: The Health Care Impact, Clinical Recognition & Treatment OptionsDocument16 pagesAtrial Flutter: The Health Care Impact, Clinical Recognition & Treatment OptionsPhillip MartinezNo ratings yet
- Dynamic Arterial Elastance To Predict Mean Arterial Pressure Decrease After Reduction of Vasopressor in Septic Shock PatientsDocument12 pagesDynamic Arterial Elastance To Predict Mean Arterial Pressure Decrease After Reduction of Vasopressor in Septic Shock PatientsAltair Monti TeslaNo ratings yet
- No Reflujo 9Document13 pagesNo Reflujo 9DenisseRangelNo ratings yet
- HRT 09000902Document6 pagesHRT 09000902boynextdoorpkyNo ratings yet
- Kontras StatinDocument10 pagesKontras Statinale_rhdNo ratings yet
- Project Presentation-Sydney StratfordDocument17 pagesProject Presentation-Sydney Stratfordapi-611918048No ratings yet
- 296 Neck of Femur Fracture Peri-Operative ManagementDocument8 pages296 Neck of Femur Fracture Peri-Operative ManagementNilam dwinilamsariNo ratings yet
- Eht 104Document9 pagesEht 104MAX ANTHONY SALAMANCA HILASACANo ratings yet
- Komplikasi Stroke PDFDocument7 pagesKomplikasi Stroke PDFJose Hady PuteraNo ratings yet
- Total Summerized EMPA STUDIES 2Document51 pagesTotal Summerized EMPA STUDIES 2EslamNo ratings yet
- Heart J: Outcome of Primary Percutaneous Coronary Intervention With Early and Late ST Resolution - Earlier Is Better!Document6 pagesHeart J: Outcome of Primary Percutaneous Coronary Intervention With Early and Late ST Resolution - Earlier Is Better!ayesha FalakNo ratings yet
- Antiplaq y HsaDocument5 pagesAntiplaq y HsaWaldemar PiñaNo ratings yet
- Haematemesis and MalenaDocument39 pagesHaematemesis and MalenaNikNo ratings yet
- 3.prof - Iman Supandiman-Prophylaxis and Treatment Thrombosis in Cancer - NewDocument39 pages3.prof - Iman Supandiman-Prophylaxis and Treatment Thrombosis in Cancer - NewpriyopanjiNo ratings yet
- Manajemen Preoperatif Pasien Dengan Terapi KoagulanDocument32 pagesManajemen Preoperatif Pasien Dengan Terapi KoagulanRaditya DidotNo ratings yet
- Oasis 5Document13 pagesOasis 5Anggita Nur Widya FebrianaNo ratings yet
- Top Trials in Gastroenterology & HepatologyFrom EverandTop Trials in Gastroenterology & HepatologyRating: 4.5 out of 5 stars4.5/5 (7)
- Cardiac Care and COVID-19: Perspectives in Medical PracticeFrom EverandCardiac Care and COVID-19: Perspectives in Medical PracticeNo ratings yet
- Clinical Assessment in Acute Heart Failure: Review ArticleDocument17 pagesClinical Assessment in Acute Heart Failure: Review ArticleAnonymous NeRC5JYiSNo ratings yet
- Altered Ketones and HFDocument13 pagesAltered Ketones and HFAnonymous NeRC5JYiSNo ratings yet
- ESC Guidelines On Cardio-Oncology - 2022Document133 pagesESC Guidelines On Cardio-Oncology - 2022nicolasNo ratings yet
- ADHF in HFpEFDocument9 pagesADHF in HFpEFAnonymous NeRC5JYiSNo ratings yet
- Advances in Managing Acute Decompensated Heart FailureDocument14 pagesAdvances in Managing Acute Decompensated Heart FailureAnonymous NeRC5JYiSNo ratings yet
- Biomarkers in HFDocument17 pagesBiomarkers in HFAnonymous NeRC5JYiSNo ratings yet
- Altered Hemodynamics and End-Organ in HFDocument15 pagesAltered Hemodynamics and End-Organ in HFAnonymous NeRC5JYiSNo ratings yet
- Acute Kidney Injury in HFDocument14 pagesAcute Kidney Injury in HFAnonymous NeRC5JYiSNo ratings yet
- Atrial Fibrilasi Dan HF - MekanismeDocument10 pagesAtrial Fibrilasi Dan HF - MekanismeAnonymous NeRC5JYiSNo ratings yet
- Target Dose Vs Target HRDocument3 pagesTarget Dose Vs Target HRAnonymous NeRC5JYiSNo ratings yet
- A Randomized Controlled Trial CCMDocument10 pagesA Randomized Controlled Trial CCMAnonymous NeRC5JYiSNo ratings yet
- Age and Atrial FibrilasiDocument8 pagesAge and Atrial FibrilasiAnonymous NeRC5JYiSNo ratings yet
- Age Risk Factors Heart FailureDocument9 pagesAge Risk Factors Heart FailureAnonymous NeRC5JYiSNo ratings yet
- ADHF HFrEFDocument14 pagesADHF HFrEFAnonymous NeRC5JYiSNo ratings yet
- Smoking and CHDDocument19 pagesSmoking and CHDAnonymous NeRC5JYiSNo ratings yet
- Calcium Channel Blockers Report PDFDocument43 pagesCalcium Channel Blockers Report PDFElyza XeNo ratings yet
- Prospect TrialDocument37 pagesProspect TrialAnonymous NeRC5JYiSNo ratings yet
- RHDDocument130 pagesRHDDeepu RajendranNo ratings yet
- ASCOT Hypertension StudyDocument12 pagesASCOT Hypertension StudyAnonymous NeRC5JYiSNo ratings yet
- Calcium Channel Blockers inDocument15 pagesCalcium Channel Blockers inAnonymous NeRC5JYiSNo ratings yet
- Pathogenic Mechanisms in Rheumatic Carditis Focus On Valvular EndotheliumDocument5 pagesPathogenic Mechanisms in Rheumatic Carditis Focus On Valvular EndotheliumAnonymous NeRC5JYiSNo ratings yet
- SARS COV2 Vaccination and MyocarditisDocument9 pagesSARS COV2 Vaccination and MyocarditisMicaela Belen LuccardiNo ratings yet
- Continuing Cardiology EducationDocument7 pagesContinuing Cardiology EducationAnonymous NeRC5JYiSNo ratings yet
- BB AND CCBDocument16 pagesBB AND CCBAnonymous NeRC5JYiSNo ratings yet
- Ehx493 P5438Document1 pageEhx493 P5438Anonymous NeRC5JYiSNo ratings yet
- Acls Algorithms Rapid RatesDocument8 pagesAcls Algorithms Rapid RatesAnonymous NeRC5JYiSNo ratings yet
- Echo Presentation - Endocrine Nefro HematoDocument27 pagesEcho Presentation - Endocrine Nefro HematoAnonymous NeRC5JYiSNo ratings yet
- ACLS Rhythms For The ACLS Algorithms: AppendixDocument32 pagesACLS Rhythms For The ACLS Algorithms: Appendixyan_ricci19100% (4)
- Proposed Diagnostic Brugada SyndromeDocument7 pagesProposed Diagnostic Brugada SyndromecyelzNo ratings yet
- OSPEDocument28 pagesOSPEsubashikNo ratings yet
- Pencegahan Dan Pengendalian Infeksi Di Rumah Sakit Dan FasyankesDocument60 pagesPencegahan Dan Pengendalian Infeksi Di Rumah Sakit Dan FasyankesNesa MuktariNo ratings yet
- Lesson Plan Personality DisorderDocument7 pagesLesson Plan Personality DisorderRaj MeghwalNo ratings yet
- Hogg and LordDocument57 pagesHogg and LordToby VueNo ratings yet
- File1-Role of Nurse in EpidemiologyDocument14 pagesFile1-Role of Nurse in EpidemiologyRufus Raj83% (23)
- Anodontia of Permanent Teeth - A Case ReportDocument3 pagesAnodontia of Permanent Teeth - A Case Reportanandsingh001No ratings yet
- Assessing Radial PulseDocument4 pagesAssessing Radial PulseMatthew RyanNo ratings yet
- Case Study Edia Ovia, NursingDocument15 pagesCase Study Edia Ovia, NursingKelly J WilsonNo ratings yet
- Clínica Oftalmológica Del Caribe (COFCA) ColombiaDocument11 pagesClínica Oftalmológica Del Caribe (COFCA) ColombiaJulio Martinez-ClarkNo ratings yet
- NP5Document19 pagesNP5Jhouleen Angelika TamNo ratings yet
- Nursing Care Plan for Skin IntegrityDocument3 pagesNursing Care Plan for Skin IntegrityCrystal Joy Misa100% (1)
- Nasal TraumaDocument5 pagesNasal TraumaRae Marie AquinoNo ratings yet
- 05 Abpg2103 Topic 1Document14 pages05 Abpg2103 Topic 1Ummu SolihahNo ratings yet
- Concept Map Epidural AbcessDocument11 pagesConcept Map Epidural Abcessapi-593859653No ratings yet
- QuizzesDocument6 pagesQuizzesJafinNo ratings yet
- 177.higher ClinicDocument18 pages177.higher Clinicabel_kayelNo ratings yet
- Thrombocytopenia in PregnancyDocument12 pagesThrombocytopenia in PregnancyzoyaNo ratings yet
- 03 The Role of "Smart" Infusion Pumps in Patient Safety PDFDocument11 pages03 The Role of "Smart" Infusion Pumps in Patient Safety PDFSaravanan NallasivanNo ratings yet
- ResumeDocument3 pagesResumeDeviprasad MahantaNo ratings yet
- Principles of Practice For Pharmaceutical CareDocument29 pagesPrinciples of Practice For Pharmaceutical CareNgetwa TzDe TheWirymanNo ratings yet
- Change Management in Health Care: Robert James Campbell, EddDocument17 pagesChange Management in Health Care: Robert James Campbell, EddeossNo ratings yet
- Exercise For Cancer PatientsDocument1 pageExercise For Cancer PatientsAdvanced PhysiotherapyNo ratings yet
- Critical Thinking Exercise NCM 106Document5 pagesCritical Thinking Exercise NCM 106Julienne Sanchez-SalazarNo ratings yet
- 12Document5 pages12yeremias setyawanNo ratings yet
- GVP Annex V AbbreviationsDocument5 pagesGVP Annex V AbbreviationsSilvia PeroniNo ratings yet
- Nursing Care Plan Infection Bartholins Duct CystDocument1 pageNursing Care Plan Infection Bartholins Duct Cystderic100% (5)
- 25 - Application of Isokinetics in Testing and RehabilitationDocument23 pages25 - Application of Isokinetics in Testing and RehabilitationCarlos GarciaNo ratings yet
- Chapter 18 - PharmDocument35 pagesChapter 18 - PharmJames PerianayagamNo ratings yet
- Effects of Kinesio Taping For Stroke Patients WithDocument8 pagesEffects of Kinesio Taping For Stroke Patients WithBias HerkawentarNo ratings yet
- Ectopic PregnancyDocument39 pagesEctopic PregnancyMuhammad SherazNo ratings yet