You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- E.R. Hooton, Tom Cooper - Desert Storm - Volume 2 - Operation Desert Storm and The Coalition Liberation of Kuwait 1991 (Middle East@War) (2021, Helion and CompanyDocument82 pagesE.R. Hooton, Tom Cooper - Desert Storm - Volume 2 - Operation Desert Storm and The Coalition Liberation of Kuwait 1991 (Middle East@War) (2021, Helion and Companydubie dubs100% (5)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Unit 3: The Catering Service Industry Topic: Catering Service Concept Digest (Discussion)Document5 pagesUnit 3: The Catering Service Industry Topic: Catering Service Concept Digest (Discussion)Justin MagnanaoNo ratings yet
- EMUS Level 1 UltrasoundDocument4 pagesEMUS Level 1 UltrasoundStphn WllngtnNo ratings yet
- Loan Agreement with Chattel Mortgage SecuredDocument6 pagesLoan Agreement with Chattel Mortgage SecuredManny DerainNo ratings yet
- SC upholds invalid donation of land shareDocument3 pagesSC upholds invalid donation of land shareAizza JopsonNo ratings yet
- College of Emergency Medicine Summative CbDDocument2 pagesCollege of Emergency Medicine Summative CbD洪靖儀No ratings yet
- Em Formative CBD 2010Document2 pagesEm Formative CBD 2010洪靖儀No ratings yet
- Content Programme Emergency Medicine Ultrasound Level 1 2014Document1 pageContent Programme Emergency Medicine Ultrasound Level 1 2014洪靖儀No ratings yet
- Child Protection Flyer November 2014Document3 pagesChild Protection Flyer November 2014洪靖儀No ratings yet
- CEM6510 MMU1385 Emergency Med HPSC18 6 12 1Document8 pagesCEM6510 MMU1385 Emergency Med HPSC18 6 12 1洪靖儀No ratings yet
- Masters in Emergency MedicineDocument1 pageMasters in Emergency MedicineRavi PattanshettyNo ratings yet
- Practical Procedures Course Poster Nove 14Document1 pagePractical Procedures Course Poster Nove 14洪靖儀No ratings yet
- Acdp VHF Guidance 2012Document99 pagesAcdp VHF Guidance 2012洪靖儀No ratings yet
- Trip Details CRQ 2014Document11 pagesTrip Details CRQ 2014洪靖儀No ratings yet
- CEM7061 PEM A3 Emailable May 2013Document1 pageCEM7061 PEM A3 Emailable May 2013洪靖儀No ratings yet
- CEM7071 Application Handbook Medical ToxicologyDocument8 pagesCEM7071 Application Handbook Medical Toxicology洪靖儀No ratings yet
- Preparing For Your ACCS ARCP 25-5-2013Document32 pagesPreparing For Your ACCS ARCP 25-5-2013洪靖儀No ratings yet
- Practical Procedures Course Poster Nove 14Document1 pagePractical Procedures Course Poster Nove 14洪靖儀No ratings yet
- Masters in Emergency MedicineDocument1 pageMasters in Emergency MedicineRavi PattanshettyNo ratings yet
- Child Protection Flyer November 2014Document3 pagesChild Protection Flyer November 2014洪靖儀No ratings yet
- Tour Summary - Trekking Mont BlancDocument2 pagesTour Summary - Trekking Mont Blanc洪靖儀No ratings yet
- 1 CSSD Seasonal Plan NEW 23 10 13 MC ApprovedDocument44 pages1 CSSD Seasonal Plan NEW 23 10 13 MC Approved洪靖儀No ratings yet
- Trip Details BILM 2014Document17 pagesTrip Details BILM 2014洪靖儀No ratings yet
- MCQ Instructions Basic Course StudentsDocument3 pagesMCQ Instructions Basic Course Students洪靖儀No ratings yet
- Acdp VHF Guidance 2012Document99 pagesAcdp VHF Guidance 2012洪靖儀No ratings yet
- Costa Rica Quest 9-Day Tour Highlights Nature, Adventure & Local CultureDocument2 pagesCosta Rica Quest 9-Day Tour Highlights Nature, Adventure & Local Culture洪靖儀No ratings yet
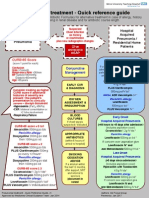
- Pneumonia treatment guide under 40 charactersDocument1 pagePneumonia treatment guide under 40 characters洪靖儀No ratings yet
- Trip Details SABL 2014Document13 pagesTrip Details SABL 2014洪靖儀No ratings yet
- Tour Summary - Trekking in The DolomitesDocument2 pagesTour Summary - Trekking in The Dolomites洪靖儀No ratings yet
- Tour Summary - Costa Rica Volcanoes & SurfDocument2 pagesTour Summary - Costa Rica Volcanoes & Surf洪靖儀No ratings yet
- Tour Summary - Morocco Active AdventureDocument2 pagesTour Summary - Morocco Active Adventure洪靖儀No ratings yet
- Smoking CessationDocument25 pagesSmoking Cessation洪靖儀No ratings yet
- MnemonicsDocument23 pagesMnemonicsmollprimeNo ratings yet
- Akriti Shrivastava CMBA2Y3-1906Document6 pagesAkriti Shrivastava CMBA2Y3-1906Siddharth ChoudheryNo ratings yet
- Basic Accounting Principles and Budgeting FundamentalsDocument24 pagesBasic Accounting Principles and Budgeting Fundamentalskebaman1986No ratings yet
- Cough: by Dr. Meghana Patil (Intern Batch 2016)Document24 pagesCough: by Dr. Meghana Patil (Intern Batch 2016)Meghana PatilNo ratings yet
- Importance and Behavior of Capital Project Benefits Factors in Practice: Early EvidenceDocument13 pagesImportance and Behavior of Capital Project Benefits Factors in Practice: Early EvidencevimalnandiNo ratings yet
- Tds Uniqflow 372s enDocument1 pageTds Uniqflow 372s enm daneshpourNo ratings yet
- Duratone eDocument1 pageDuratone eandreinalicNo ratings yet
- BVM Type B Casing Tong ManualDocument3 pagesBVM Type B Casing Tong ManualJuan Gabriel GomezNo ratings yet
- Office of The Protected Area Superintendent: Mt. Matutum Protected LandscapeDocument3 pagesOffice of The Protected Area Superintendent: Mt. Matutum Protected LandscapeNurah LaNo ratings yet
- People VS Yancon-DumacasDocument2 pagesPeople VS Yancon-Dumacasvincent nifasNo ratings yet
- OTA710C User ManualDocument32 pagesOTA710C User ManualEver Daniel Barreto Rojas100% (2)
- The Importance of Personal Protective Equipment in Pesticide App 2018Document4 pagesThe Importance of Personal Protective Equipment in Pesticide App 2018Anees MalikNo ratings yet
- Black Bruin Hydraulic Motors On-Demand Wheel Drives EN CDocument11 pagesBlack Bruin Hydraulic Motors On-Demand Wheel Drives EN CDiego AlbarracinNo ratings yet
- Philips Lighting Annual ReportDocument158 pagesPhilips Lighting Annual ReportOctavian Andrei NanciuNo ratings yet
- CS547Document11 pagesCS547Usman Suleman AhmadNo ratings yet
- Education, A Vital Principle For Digital Library Development in IranDocument23 pagesEducation, A Vital Principle For Digital Library Development in Iranrasuli9No ratings yet
- Training Prospectus 2020 WebDocument89 pagesTraining Prospectus 2020 Webamila_vithanageNo ratings yet
- ION8650 DatasheetDocument11 pagesION8650 DatasheetAlthaf Axel HiroshiNo ratings yet
- Rbalance Rotor Balancing ProcedureDocument2 pagesRbalance Rotor Balancing ProcedureBradley NelsonNo ratings yet
- Fuel Pumps Left in Off PositionDocument7 pagesFuel Pumps Left in Off PositionherbuelNo ratings yet
- Microsoft Windows 98 Second Edition README For Tips and Tricks, April 1999Document8 pagesMicrosoft Windows 98 Second Edition README For Tips and Tricks, April 1999scriNo ratings yet
- S-S-, AXXX XXX 008 (BIA Sept. 15, 2017)Document7 pagesS-S-, AXXX XXX 008 (BIA Sept. 15, 2017)Immigrant & Refugee Appellate Center, LLCNo ratings yet
- 2017 Advanced Computer Networks Homework 1Document6 pages2017 Advanced Computer Networks Homework 1Fadhli RahimNo ratings yet
- Dimetra Tetra System White PaperDocument6 pagesDimetra Tetra System White PapermosaababbasNo ratings yet
- Section 2 in The Forest (Conservation) Act, 1980Document1 pageSection 2 in The Forest (Conservation) Act, 1980amit singhNo ratings yet
- GA 7 Parts ManualDocument565 pagesGA 7 Parts ManualDave SchallNo ratings yet
- Reconciling Informal and Formal TradeDocument194 pagesReconciling Informal and Formal TradeBaterias BateriasNo ratings yet