You might also like
- EBM - 5. Adrenal DisordersDocument101 pagesEBM - 5. Adrenal DisordersBRI KUNo ratings yet
- Myoma UteriDocument21 pagesMyoma UteriLangitBiruNo ratings yet
- Olds Maternal Newborn Nursing and Womens Health Across The Lifespan 9th Edition Davidson Test BankDocument29 pagesOlds Maternal Newborn Nursing and Womens Health Across The Lifespan 9th Edition Davidson Test Bankstarostyadjustaged5p100% (27)
- Block 6 Test Human ReproductionDocument4 pagesBlock 6 Test Human ReproductionJohn OsborneNo ratings yet
- Hormon GDSDocument23 pagesHormon GDSBRI KUNo ratings yet
- Case Study GDM Complete 2017Document34 pagesCase Study GDM Complete 2017GANESANNo ratings yet
- Updated - DRAFT - MATRIKS APKK - R RSDocument598 pagesUpdated - DRAFT - MATRIKS APKK - R RSmarsella annaNo ratings yet
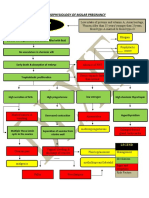
- Partial Mole or Complete Mole: Pathophysiology of Molar PregnancyDocument1 pagePartial Mole or Complete Mole: Pathophysiology of Molar PregnancyKristian Karl Bautista Kiw-isNo ratings yet
- Advantages and Disadvantages of Family PlanningDocument12 pagesAdvantages and Disadvantages of Family PlanningMARIE EYASNo ratings yet
- Abnormal Uterine BleedingDocument4 pagesAbnormal Uterine BleedingAmellyn Reyes0% (1)
- Oral Revalida - H-MoleDocument1 pageOral Revalida - H-MoleMary Loise Villegas0% (1)
- Case Study (Aub)Document16 pagesCase Study (Aub)Lucila Lugo0% (2)
- Post Abortion CareDocument35 pagesPost Abortion CareNatukunda DianahNo ratings yet
- Hydatidiform Mole - OverviewDocument4 pagesHydatidiform Mole - Overviewannmanalad9438No ratings yet
- Hyperbilirubinemia Case StudyDocument7 pagesHyperbilirubinemia Case Studyr_ramos0759No ratings yet
- Ectopic PregnancyDocument26 pagesEctopic PregnancysandhyakrishnanNo ratings yet
- 5 - Abortion or MiscarriageDocument43 pages5 - Abortion or Miscarriageasifdawar2011No ratings yet
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Community Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCommunity Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Case Study Missed Miscarriage Dilation and CurettageDocument48 pagesCase Study Missed Miscarriage Dilation and CurettageEsther Ellise AbundoNo ratings yet
- AbortionDocument28 pagesAbortionjeanpesky100% (4)
- OBG DrugsDocument30 pagesOBG DrugsSANANo ratings yet
- Neonatal Case Presentation 1Document5 pagesNeonatal Case Presentation 1Rexelle RamosNo ratings yet
- Ectopic PregnancyDocument11 pagesEctopic PregnancyPrincess BalloNo ratings yet
- Intrapartum CareDocument14 pagesIntrapartum CareChristian80% (5)
- Case Report Ca Cervix PDFDocument44 pagesCase Report Ca Cervix PDFBianca PinkyNo ratings yet
- Shoulder DystociaDocument20 pagesShoulder DystociaFaridahMaksumNo ratings yet
- Preeclampsia, HELLP Syndrome, Eclampsia and other Hypertensive Disorders of PregnancyFrom EverandPreeclampsia, HELLP Syndrome, Eclampsia and other Hypertensive Disorders of PregnancyRating: 2 out of 5 stars2/5 (1)
- Pyelonephritis (Final Case)Document59 pagesPyelonephritis (Final Case)Marasmus Kwashiorkor100% (1)
- Hypertension in Pregnancy CompiledDocument67 pagesHypertension in Pregnancy CompiledRaiza Love Caparas-PablicoNo ratings yet
- Health Talk TopicsDocument3 pagesHealth Talk Topicsvarshasharma0562% (13)
- Benign Breast DisordersDocument42 pagesBenign Breast DisordersBRI KUNo ratings yet
- OligohydramniosDocument4 pagesOligohydramniossalamredNo ratings yet
- PPROMDocument63 pagesPPROMSaraMohammedNo ratings yet
- JMDocument45 pagesJMDana Fajardo RezanoNo ratings yet
- Pre-eclampsia, (Pregnancy with Hypertension And Proteinuria) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPre-eclampsia, (Pregnancy with Hypertension And Proteinuria) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- GASTROSCHISISDocument4 pagesGASTROSCHISISVin Custodio100% (1)
- Case Study On Pregnancy Induced Hypertension (PIH) : University of Northern Philippines College of NursingDocument42 pagesCase Study On Pregnancy Induced Hypertension (PIH) : University of Northern Philippines College of Nursing3B NOVIDA, ALEYA G.No ratings yet
- Post Partum HemorrhageDocument40 pagesPost Partum HemorrhageGita GirsangNo ratings yet
- Ectopic Pregnancy - CSDocument14 pagesEctopic Pregnancy - CSMASII100% (1)
- Incomplete Abortion: A Mini Case Study OnDocument22 pagesIncomplete Abortion: A Mini Case Study OnSunny MujmuleNo ratings yet
- Case PresentationDocument50 pagesCase Presentationapi-19762967No ratings yet
- DEFINITION: Abortion Is The Expulsion or Extraction From Its MotherDocument10 pagesDEFINITION: Abortion Is The Expulsion or Extraction From Its MothermOHAN.SNo ratings yet
- Molar Pregnancy: November 2018 Jis Dungca, Delos Santos, CrisostomoDocument99 pagesMolar Pregnancy: November 2018 Jis Dungca, Delos Santos, CrisostomoDarnell DelgadoNo ratings yet
- Incomplete AbortionDocument18 pagesIncomplete AbortionAra DirganNo ratings yet
- Case Study PreeclampsiaDocument3 pagesCase Study PreeclampsiaRima Christa Ulin SitepuNo ratings yet
- A Nursing Case Study On EctopicPregnancy PDFDocument60 pagesA Nursing Case Study On EctopicPregnancy PDFSteffiNo ratings yet
- Case StudyDocument19 pagesCase Studywella goNo ratings yet
- Polyhydraminos and OligohydraminosDocument11 pagesPolyhydraminos and OligohydraminosMelissa Catherine ChinNo ratings yet
- Pyloric StenosisDocument5 pagesPyloric Stenosisensoooooooooo100% (1)
- Case Pres AutosavedDocument21 pagesCase Pres AutosavedJaysellePuguonTabijeNo ratings yet
- Ectopic Pregnancy: DR .Urmila KarkiDocument27 pagesEctopic Pregnancy: DR .Urmila KarkiBasudev chNo ratings yet
- 35 - Retained PlacentaDocument11 pages35 - Retained Placentadr_asalehNo ratings yet
- Pre EclampsiaDocument13 pagesPre EclampsiaEniamrahs DnalonNo ratings yet
- Management Placenta PreviaDocument24 pagesManagement Placenta PreviaMuhammad RifaldiNo ratings yet
- What Is A Retained Placenta?Document4 pagesWhat Is A Retained Placenta?Baharudin Yusuf Ramadhani0% (1)
- Intrauterine Growth Restriction IUGR: TH THDocument2 pagesIntrauterine Growth Restriction IUGR: TH THZahra AlaradiNo ratings yet
- Case Study Benign Tumors of The Uterus: MyomaDocument3 pagesCase Study Benign Tumors of The Uterus: MyomaToto RyanNo ratings yet
- UTERINE PROLAPSE - Case ReportDocument3 pagesUTERINE PROLAPSE - Case ReportIOSRjournalNo ratings yet
- Myoma Final Power PointDocument45 pagesMyoma Final Power Pointicesexy100% (1)
- Case3 Case StudyDocument6 pagesCase3 Case StudyKrizzia Angela BacotocNo ratings yet
- Case - Eclampsia FinalDocument84 pagesCase - Eclampsia FinalKimberley Anne SantosNo ratings yet
- Case Study of Cesarean SectionDocument9 pagesCase Study of Cesarean SectionErika Joy Imperio0% (1)
- Hydatidiform Mole Study GuideDocument4 pagesHydatidiform Mole Study GuideCarl Elexer Cuyugan AnoNo ratings yet
- Hyper Emesis GravidarumDocument22 pagesHyper Emesis Gravidarumchandu ranaNo ratings yet
- Biliary AtresiaDocument8 pagesBiliary AtresiaBrooke MauriNo ratings yet
- Hyperemesis GravidarumDocument36 pagesHyperemesis GravidarumjanissNo ratings yet
- Spontaneous AbortionDocument8 pagesSpontaneous Abortionsaber_fate_11No ratings yet
- Final Case Study SLDocument17 pagesFinal Case Study SLCharmie Mei Paredes-RoqueNo ratings yet
- Case Study in ObwardDocument6 pagesCase Study in Obwardcharles_florendo25100% (3)
- Gastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandGastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Lecture: Histology of Cartilage and BoneDocument46 pagesLecture: Histology of Cartilage and BoneBRI KUNo ratings yet
- Blood Transfusion: Hemato - Oncology Division Departement of Child Health Medical School University of Sumatera UtaraDocument28 pagesBlood Transfusion: Hemato - Oncology Division Departement of Child Health Medical School University of Sumatera UtaraBRI KUNo ratings yet
- K6-Nutrition and Bone HealthDocument30 pagesK6-Nutrition and Bone HealthBRI KU0% (1)
- Diarrhoea (Part 2)Document31 pagesDiarrhoea (Part 2)BRI KUNo ratings yet
- Necrotizing Enterocolitis: Department of Childhealth, School of Medicine, University of North Sumatera MedanDocument17 pagesNecrotizing Enterocolitis: Department of Childhealth, School of Medicine, University of North Sumatera MedanBRI KUNo ratings yet
- IldDocument13 pagesIldBRI KUNo ratings yet
- Fluid, Electrolyte, and Acid-Base BalanceDocument50 pagesFluid, Electrolyte, and Acid-Base BalanceBRI KUNo ratings yet
- Theory For Reading Comprehension: A Brief DiscussionDocument6 pagesTheory For Reading Comprehension: A Brief DiscussionBRI KUNo ratings yet
- DR Hayu Lestari Haryono Spog: Divisi Feto Maternal FK Usu /rs HamDocument26 pagesDR Hayu Lestari Haryono Spog: Divisi Feto Maternal FK Usu /rs HamBRI KUNo ratings yet
- Lung Pathology: Respiratory System BlockDocument83 pagesLung Pathology: Respiratory System BlockBRI KUNo ratings yet
- DR Hayu Lestari Haryono Spog: Divisi Feto Maternal FK Usu /rs HamDocument26 pagesDR Hayu Lestari Haryono Spog: Divisi Feto Maternal FK Usu /rs HamBRI KUNo ratings yet
- Kanker Paru (Lung Cancer) : Blok Onkology FK UhnDocument48 pagesKanker Paru (Lung Cancer) : Blok Onkology FK UhnBRI KUNo ratings yet
- Tension-Type Headache: ReferencesDocument1 pageTension-Type Headache: ReferencesBRI KUNo ratings yet
- Bayi Baru LahirDocument43 pagesBayi Baru LahirBRI KUNo ratings yet
- The Uses and Limitations of The Fetal Biophysical Profile.Document18 pagesThe Uses and Limitations of The Fetal Biophysical Profile.Diego Ortecho100% (1)
- Patrick Perez - Chapter Xxx-1Document13 pagesPatrick Perez - Chapter Xxx-1Jayrald Delos SantosNo ratings yet
- Options For Medical Treatment of Myomas: Beth W. Rackow, MD, Aydin Arici, MDTDocument14 pagesOptions For Medical Treatment of Myomas: Beth W. Rackow, MD, Aydin Arici, MDTDimas YudhistiraNo ratings yet
- Roxipan (Oxytocin) - Drug StudyDocument4 pagesRoxipan (Oxytocin) - Drug StudyIzza DeloriaNo ratings yet
- Common Obstetrics Case ScenariosDocument10 pagesCommon Obstetrics Case ScenariosPeter LeeNo ratings yet
- Missed AbortionDocument5 pagesMissed AbortionDesta MarpaungNo ratings yet
- 2008-Sci-039 Rop Append ADocument2 pages2008-Sci-039 Rop Append Aavram_elenaNo ratings yet
- Forceps DeliveryDocument30 pagesForceps DeliveryKozang Meong lhaNo ratings yet
- Jurnal 2Document7 pagesJurnal 2mellvinNo ratings yet
- Health Status of Rural Women in OdishaDocument10 pagesHealth Status of Rural Women in OdishaEditor IJTSRDNo ratings yet
- Abortion: PathophysiologyDocument3 pagesAbortion: PathophysiologyEdmund Lominoque LamelaNo ratings yet
- Menstrual Suppression Using Oral Contraceptives by Female Hajj PilgrimsDocument4 pagesMenstrual Suppression Using Oral Contraceptives by Female Hajj PilgrimsSony Eka NugrahaNo ratings yet
- CCH Gynaecology SyllabusDocument2 pagesCCH Gynaecology Syllabusanon_631988652No ratings yet
- Group 2: Behavioral MethodsDocument17 pagesGroup 2: Behavioral Methodsrockzme_babyNo ratings yet
- Antenatal AssessmentDocument24 pagesAntenatal AssessmentIshrat PatelNo ratings yet
- Ectopic and Molar PregnancyDocument22 pagesEctopic and Molar Pregnancyapi-381845148No ratings yet
- Course Information For Current Semester/Term: Maklumat Kursus Untuk Semester/Penggal SemasaDocument5 pagesCourse Information For Current Semester/Term: Maklumat Kursus Untuk Semester/Penggal SemasaNurul IrhamnaNo ratings yet
- Management of Second-Stage LaborDocument34 pagesManagement of Second-Stage LaborAshwini TirkeyNo ratings yet
- Amazing Facts About Human Reproductive SystemDocument3 pagesAmazing Facts About Human Reproductive SystemDaniel C. DequiñaNo ratings yet
- BibliographyDocument17 pagesBibliographyChristian D BlessingNo ratings yet
- Lochia Patterns Among Normal Women: A Systematic ReviewDocument5 pagesLochia Patterns Among Normal Women: A Systematic Reviewasm obginNo ratings yet