You might also like
- Cerebellum and Brain Stem: DR Asim Shrestha SRCC Ped Neuro Fellow MumbaiDocument71 pagesCerebellum and Brain Stem: DR Asim Shrestha SRCC Ped Neuro Fellow MumbaiAsim ShresthaNo ratings yet
- Diagnostic Approach To HeadacheDocument7 pagesDiagnostic Approach To HeadachedanlaytonNo ratings yet
- John Christy Hard Gainer Articles CompilationDocument235 pagesJohn Christy Hard Gainer Articles CompilationGuiye MarisiNo ratings yet
- Cardiovascular System: More Than Just The HeartDocument34 pagesCardiovascular System: More Than Just The HearteliseudesafateNo ratings yet
- 21-Spinal Cord TractsDocument23 pages21-Spinal Cord TractsALFAHRUL CAHYADINo ratings yet
- BBB Nov-Dec 2023 Workout PlanDocument17 pagesBBB Nov-Dec 2023 Workout Planjfiorav6100% (1)
- Clinical Approach To Brainstem LesionsDocument10 pagesClinical Approach To Brainstem LesionsJosé SánchezNo ratings yet
- Presented By: VIVEK DEVDocument38 pagesPresented By: VIVEK DEVFranchesca LugoNo ratings yet
- Head and Neck AnswersDocument15 pagesHead and Neck AnswersANDRE MANo ratings yet
- Endocrine System ReviewerDocument23 pagesEndocrine System ReviewerKimberly Joy GregorioNo ratings yet
- Compiled Questions - Head and Neck (Anatomy)Document2 pagesCompiled Questions - Head and Neck (Anatomy)Joezer Gumangan VeranoNo ratings yet
- Degeneration & Regeneration of Nerve FibreDocument29 pagesDegeneration & Regeneration of Nerve FibreSana FatimaNo ratings yet
- The Midbrain and Important ConnectionsDocument118 pagesThe Midbrain and Important ConnectionsBaguma MichaelNo ratings yet
- ComaDocument42 pagesComaTapash GopeNo ratings yet
- PPTDocument61 pagesPPTRheal P EsmailNo ratings yet
- Pain PathwaysDocument45 pagesPain PathwaysKabirNo ratings yet
- Physiology of Hearing & BalanceDocument41 pagesPhysiology of Hearing & BalanceSudhir BayyaNo ratings yet
- 1.physiology of Nervous System DR Hasnain Northwest Univerty PeshawarDocument27 pages1.physiology of Nervous System DR Hasnain Northwest Univerty PeshawarHasin's QueenNo ratings yet
- Medical Power PointDocument105 pagesMedical Power PointSarah Dwitya100% (1)
- Headache: Prepared byDocument23 pagesHeadache: Prepared byjawad_ahmedNo ratings yet
- Centric Relation and Condylar Movement: Anatomic MechanismDocument11 pagesCentric Relation and Condylar Movement: Anatomic MechanismJoohi SharmaNo ratings yet
- Cerebrovascular AccidentDocument8 pagesCerebrovascular AccidentKarina CastilloNo ratings yet
- 397.001 - Orthopedics) Rotator Cuff TearDocument11 pages397.001 - Orthopedics) Rotator Cuff Tearvkpremiyahoo.comNo ratings yet
- 9.superficial Heating ModalitiesDocument11 pages9.superficial Heating ModalitiesFaisal Mehboob100% (2)
- The-Skull by Dr. Phan SandethDocument65 pagesThe-Skull by Dr. Phan SandethTith Sunny100% (2)
- Obi Vincent Workout PDFDocument2 pagesObi Vincent Workout PDFPedro Silva50% (2)
- Feb 5 2020 - Endocrine System g10Document5 pagesFeb 5 2020 - Endocrine System g10Lymberth BenallaNo ratings yet
- BBB Month 26 Workout LogDocument8 pagesBBB Month 26 Workout LogluniblueNo ratings yet
- HemiplegiaDocument30 pagesHemiplegiasarguss14100% (1)
- Neuroanatomy Questions Units 1-8Document19 pagesNeuroanatomy Questions Units 1-8GoNo ratings yet
- Vertebral Arteries, and Their Divisions. Arteries Fuse To Form The Basilar ArteryDocument6 pagesVertebral Arteries, and Their Divisions. Arteries Fuse To Form The Basilar Arterymurali_bharadwazNo ratings yet
- Exam A-3Document11 pagesExam A-3yapues87No ratings yet
- Chapter 24 Urinary BladderDocument42 pagesChapter 24 Urinary BladderMACON824No ratings yet
- DR LinDocument3 pagesDR Linperdurabo2No ratings yet
- Openings in The Skull Bone of The Skull Structures TransmittedDocument19 pagesOpenings in The Skull Bone of The Skull Structures TransmittedMacy Peralta100% (1)
- CRANIOVETEBRALJUNCTIONDocument130 pagesCRANIOVETEBRALJUNCTIONdrarunrao100% (1)
- Mptregulations 2010Document81 pagesMptregulations 2010jayababuNo ratings yet
- Thoracic Inlet Syndrome and Cervical RibDocument28 pagesThoracic Inlet Syndrome and Cervical RibRabin DasNo ratings yet
- BSC Nursing - Cardiac OutputDocument10 pagesBSC Nursing - Cardiac OutputDIKSHA RANI DEKANo ratings yet
- Head TraumaDocument22 pagesHead TraumaEllsay AliceNo ratings yet
- HEMOPHILIADocument27 pagesHEMOPHILIAr DNo ratings yet
- Internal CapsuleDocument25 pagesInternal CapsuleMadan KumarNo ratings yet
- Oculomotor Nerve: Components Main Action SuppliesDocument10 pagesOculomotor Nerve: Components Main Action Suppliesdisha1990No ratings yet
- Biomechanics of Peripheral and Spinal Nerve RootsDocument86 pagesBiomechanics of Peripheral and Spinal Nerve RootsJawad HassanNo ratings yet
- SkullDocument48 pagesSkulldavid100% (1)
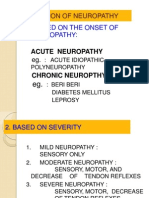
- Classification of NeuropathyDocument16 pagesClassification of NeuropathysekiannNo ratings yet
- PONS: NeuroanatomyDocument20 pagesPONS: NeuroanatomyHassan IlyasNo ratings yet
- CRANIAL Nerves - ExaminationDocument14 pagesCRANIAL Nerves - ExaminationMoussa FarhatNo ratings yet
- Diseases of The Spinal CordDocument89 pagesDiseases of The Spinal CordLolla SinwarNo ratings yet
- Facial Nerve Palsy: Dr. Saud AlromaihDocument74 pagesFacial Nerve Palsy: Dr. Saud AlromaihChandra ManapaNo ratings yet
- Regulation of Respiration During ExerciseDocument19 pagesRegulation of Respiration During ExerciseBaljeet SinghNo ratings yet
- Acute Inflammation (Vascular Changes) - 1Document33 pagesAcute Inflammation (Vascular Changes) - 1Ramesh KumarNo ratings yet
- Chapter 10 - Trigeminal NeuralgiaDocument5 pagesChapter 10 - Trigeminal NeuralgiaMuhammad IkbarNo ratings yet
- Head InjuryDocument10 pagesHead InjuryMelia SariNo ratings yet
- Lung SurgeriesDocument43 pagesLung SurgeriesSereinNo ratings yet
- Anesthesia MachinesDocument4 pagesAnesthesia MachinesEmilio CánepaNo ratings yet
- Nerve Supply of Head and NeckDocument74 pagesNerve Supply of Head and NeckDr Komal GhiyaNo ratings yet
- Future Challenges in Physical TherapyDocument9 pagesFuture Challenges in Physical TherapyIqra KanwalNo ratings yet
- Blood Supply of BrainDocument2 pagesBlood Supply of BrainvmagtotoNo ratings yet
- Ocular InjuryDocument46 pagesOcular InjurysnyNo ratings yet
- Transverse MyelitisDocument19 pagesTransverse MyelitisAnonymous YHQmN8a01100% (1)
- Upper Limb MusclesDocument43 pagesUpper Limb MusclesIqraNo ratings yet
- Cardiac OutputDocument31 pagesCardiac OutputanojNo ratings yet
- Neuro PDFDocument12 pagesNeuro PDFVishnu Krsh100% (1)
- CVADocument13 pagesCVAAmlan jyoti thanapatiNo ratings yet
- Blood Supply of The BrainDocument11 pagesBlood Supply of The Brainneleh grayNo ratings yet
- Norma Basalis: Inferior Aspect of SkullDocument33 pagesNorma Basalis: Inferior Aspect of Skullkavya0% (1)
- Cranial Nerve I - Olfactory NerveDocument6 pagesCranial Nerve I - Olfactory NerveAysha AishaNo ratings yet
- Cranial NervesDocument40 pagesCranial NervesugochukwuNo ratings yet
- Physiology 102Document5 pagesPhysiology 102Javed AkhlaqNo ratings yet
- Paschimottanasana 001 Paschimottanasana 002Document1 pagePaschimottanasana 001 Paschimottanasana 002Karisma SenapatiNo ratings yet
- The Nervous System: Anatomy & PhysiologyDocument30 pagesThe Nervous System: Anatomy & PhysiologyDrAvinash NandanNo ratings yet
- Lumbar Radiculopathy SyndromeDocument2 pagesLumbar Radiculopathy SyndromeAqsa KiranNo ratings yet
- English Language & Comprehension: InstructionsDocument6 pagesEnglish Language & Comprehension: Instructionssunny kumarNo ratings yet
- Upper LimbDocument20 pagesUpper Limbhafsah sidi abdullahiNo ratings yet
- The Muscular System: Essentials of Anatomy & PhysiologyDocument74 pagesThe Muscular System: Essentials of Anatomy & PhysiologySwetaNo ratings yet
- Amraz e QalbDocument15 pagesAmraz e Qalbdrmshiffa0% (2)
- Dance Core Strengthening ExercisesDocument2 pagesDance Core Strengthening ExercisesgenedandreaNo ratings yet
- Examination of The Cranial NervesDocument23 pagesExamination of The Cranial NervesMunawar AcehNo ratings yet
- Mucosa Oral DermatologoDocument537 pagesMucosa Oral DermatologoKAREN ESTHER CAPACOILA GRANADOSNo ratings yet
- Kahoot 1Document6 pagesKahoot 1Nida RidzuanNo ratings yet
- Urinary Frequency in PregnancyDocument14 pagesUrinary Frequency in PregnancyTanya WilliamsNo ratings yet
- Physical Assessment Checklist For DutyDocument9 pagesPhysical Assessment Checklist For DutyRena EjorcadasNo ratings yet
- Krok 1 - 2015 (Physiology)Document28 pagesKrok 1 - 2015 (Physiology)Harsh NimavatNo ratings yet
- Imp Questions ANATOMY - 221113 - 090816Document7 pagesImp Questions ANATOMY - 221113 - 090816ashmita pandaNo ratings yet
- Practical 1 XII YogaDocument10 pagesPractical 1 XII YogaNamanNo ratings yet
- Nervous System Endocrine System and Reproductive SystemDocument5 pagesNervous System Endocrine System and Reproductive SystemMcdaryl Inmenzo Lleno50% (2)
- Case IhDocument43 pagesCase IhChie Hyun-AeNo ratings yet
- Posterior Pelvic Tilt Routine PMCDocument7 pagesPosterior Pelvic Tilt Routine PMCldletkemanNo ratings yet
- Is Orthodontic Treatment Without Premolar Extractions Always Non-Extraction Treatment?Document6 pagesIs Orthodontic Treatment Without Premolar Extractions Always Non-Extraction Treatment?Hafaifa TaiebNo ratings yet