You might also like
- Cystatin C As An Early Marker of Diabetic Nephropathy in Nigerian Adults With Type 2 DiabetesDocument9 pagesCystatin C As An Early Marker of Diabetic Nephropathy in Nigerian Adults With Type 2 Diabetesijmb333No ratings yet
- Dr. Dr. Agus S. Kosasih., SP - PK (K), MARS - ESR in Hematology Malignancy 29042022Document57 pagesDr. Dr. Agus S. Kosasih., SP - PK (K), MARS - ESR in Hematology Malignancy 29042022Rini WidyantariNo ratings yet
- DR - Dr. Tri Ratnaningsih, MKes, SPPK (K) - Talasemia Joglo 2021Document20 pagesDR - Dr. Tri Ratnaningsih, MKes, SPPK (K) - Talasemia Joglo 2021Eldo TaufilaNo ratings yet
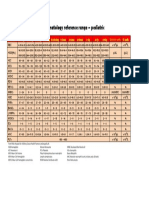
- Hematology Reference RangeDocument1 pageHematology Reference RangeNheeya WarzNo ratings yet
- BilirubinDocument5 pagesBilirubinVictor EkutaNo ratings yet
- HCV diagnostic and health care worker managementDocument36 pagesHCV diagnostic and health care worker managementLaboratorium Ansari SalehNo ratings yet
- Tutor Imun HBsAg KuantitatifDocument27 pagesTutor Imun HBsAg Kuantitatifv_mayasari100% (1)
- Prenatal Screening: HM Sulchan Sofoewan Divisi Feto-Maternal Bagian Obstetri Dan Ginekologi FK UGMDocument54 pagesPrenatal Screening: HM Sulchan Sofoewan Divisi Feto-Maternal Bagian Obstetri Dan Ginekologi FK UGMTahta PambudiNo ratings yet
- EritrositDocument12 pagesEritrositNatasya HerinNo ratings yet
- Laboratory Hemostatic DisordersDocument41 pagesLaboratory Hemostatic DisordersYohanna SinuhajiNo ratings yet
- New Red Blood Cell and Reticulocyte Parameters and Reference Values For Healthy Individuals and in Chronic Kidney Disease.Document8 pagesNew Red Blood Cell and Reticulocyte Parameters and Reference Values For Healthy Individuals and in Chronic Kidney Disease.Alberto MarcosNo ratings yet
- FACSDocument24 pagesFACSMudit MisraNo ratings yet
- What'S New in Treatment Monitoring: Viral Load and Cd4 TestingDocument2 pagesWhat'S New in Treatment Monitoring: Viral Load and Cd4 TestingRina ErlinaNo ratings yet
- Week10 Immunohematologypart1Document158 pagesWeek10 Immunohematologypart1Micah Daniel TapiaNo ratings yet
- MyelomaDocument71 pagesMyelomaHeldhi Yonathan PutraNo ratings yet
- Apus Darah Tepi, Amaylia OehadianDocument55 pagesApus Darah Tepi, Amaylia OehadianJeffry Chandra TjahayadiNo ratings yet
- Hematology 2Document58 pagesHematology 2Laboratorium Ansari SalehNo ratings yet
- 3-1 - Ida ParwatiDocument34 pages3-1 - Ida ParwatiFaisal NurlanNo ratings yet
- Feritin TestDocument9 pagesFeritin TestCharles SibagariangNo ratings yet
- BCR - Abl Oncogene: Pramod DarvinDocument16 pagesBCR - Abl Oncogene: Pramod DarvinPramod DarvinNo ratings yet
- ThalassemiaDocument45 pagesThalassemiaShella Novita100% (3)
- Hematology Reference Values in Indonesian ChildrenDocument16 pagesHematology Reference Values in Indonesian ChildrenRini WidyantariNo ratings yet
- Hemoglobin Opa ThiesDocument34 pagesHemoglobin Opa ThiesFebri fitraNo ratings yet
- Biomarker Lactate (DR Agus Kosasih SPPK)Document31 pagesBiomarker Lactate (DR Agus Kosasih SPPK)sunterjaya1 sunterjaya1No ratings yet
- Tes Lab Pada Peny Infeksi Dan Tropis (Lebih Singkat)Document71 pagesTes Lab Pada Peny Infeksi Dan Tropis (Lebih Singkat)Monazzt AsshagabNo ratings yet
- Oncogenesis Topic by Laraib FiazDocument23 pagesOncogenesis Topic by Laraib FiazLaraib FiazNo ratings yet
- CRP vs ESR Clinical AuditDocument12 pagesCRP vs ESR Clinical AuditLuke LauNo ratings yet
- Multiple Myeloma OverviewDocument52 pagesMultiple Myeloma OverviewanmegpraNo ratings yet
- Para Protein Emi ADocument14 pagesPara Protein Emi AMohamoud MohamedNo ratings yet
- CEA Medical Laboratory StandardsDocument20 pagesCEA Medical Laboratory StandardsAdv Manish Gudadhe PatilNo ratings yet
- Guidelines For The Clinical Management of ThalassemiaDocument205 pagesGuidelines For The Clinical Management of ThalassemiaAmalia Muchammad BafagihNo ratings yet
- Hemostasis Dan Koagulasi: DR - Fedelia Raya, M.Kes, SPPK Bagian Patologi Klinik Fk-UhoDocument18 pagesHemostasis Dan Koagulasi: DR - Fedelia Raya, M.Kes, SPPK Bagian Patologi Klinik Fk-UhoToraoNo ratings yet
- Laboratory Technology: Flow Cytometry Principles and Application in HematologyDocument40 pagesLaboratory Technology: Flow Cytometry Principles and Application in HematologyYuli RohmaNo ratings yet
- Laboratory Management 1Document33 pagesLaboratory Management 1Laboratorium Ansari SalehNo ratings yet
- CA125: A Marker for Ovarian Cancer Detection and MonitoringDocument3 pagesCA125: A Marker for Ovarian Cancer Detection and Monitoringडा. सत्यदेव त्यागी आर्यNo ratings yet
- Ospe Patologi Klinik - 2014Document32 pagesOspe Patologi Klinik - 2014albertrianthoNo ratings yet
- DR Dewi Yennita Sari SPPK Mendapatkan PME Kimia Klinik Yang Baik. Webinar INAEQAS KIMIA PDSPatKLIn 29802020-1 PDFDocument36 pagesDR Dewi Yennita Sari SPPK Mendapatkan PME Kimia Klinik Yang Baik. Webinar INAEQAS KIMIA PDSPatKLIn 29802020-1 PDFRini WidyantariNo ratings yet
- Pancytopenia As Initial Presentation of Acute Lymphoblastic Leukemia and Its Associationwith Bone MarrowresponseDocument6 pagesPancytopenia As Initial Presentation of Acute Lymphoblastic Leukemia and Its Associationwith Bone MarrowresponseIJAR JOURNALNo ratings yet
- PEMERIKSAAN LABORATORIUM UNTUK MONITORING INFEKSI HUMAN IMMUNODEFICIENCY VIRUSDocument33 pagesPEMERIKSAAN LABORATORIUM UNTUK MONITORING INFEKSI HUMAN IMMUNODEFICIENCY VIRUSMustakim DuharingNo ratings yet
- Pediatric Transfusion Risks and GuidelinesDocument57 pagesPediatric Transfusion Risks and GuidelinesDR.RAJESWARI SUBRAMANIYANNo ratings yet
- Hematology AnalyzerDocument35 pagesHematology AnalyzerSeemab AhmadNo ratings yet
- Pemeriksaan Laboratorium Hormon Tiroid: Oleh: Dr. Diah Hermayanti, SPPKDocument16 pagesPemeriksaan Laboratorium Hormon Tiroid: Oleh: Dr. Diah Hermayanti, SPPKZulfan RifqiawanNo ratings yet
- Thrombosis and Embolism UPR 1Document45 pagesThrombosis and Embolism UPR 1Juan Ortega PutraNo ratings yet
- Perbandingan Metode Pada Pemeriksaan Penggolongan Darah Abo Dan RhesusDocument2 pagesPerbandingan Metode Pada Pemeriksaan Penggolongan Darah Abo Dan RhesusafniridwanNo ratings yet
- Test Fs Ginjal & Urinalysis 2018Document53 pagesTest Fs Ginjal & Urinalysis 2018RuriNo ratings yet
- Bsis25 Tibc 2018Document4 pagesBsis25 Tibc 2018Houssam DjeradNo ratings yet
- Rapid Plasma Reagin TestDocument16 pagesRapid Plasma Reagin Testagoston_cristinaNo ratings yet
- Haematologist-Reviewed Peripheral Blood Smear in PDocument6 pagesHaematologist-Reviewed Peripheral Blood Smear in PElba AlvarezNo ratings yet
- Daftar Nilai Normal Pemeriksaan Laboratorium RsiaDocument4 pagesDaftar Nilai Normal Pemeriksaan Laboratorium Rsialab mutiara bundaNo ratings yet
- Doac Vs LMWHDocument6 pagesDoac Vs LMWHTry Enos OktafianNo ratings yet
- Introduction To Labeled ImmunoassayDocument26 pagesIntroduction To Labeled ImmunoassayJohn Alfrey Dondiego PuebloNo ratings yet
- Flagging and Result Interpretation-1Document41 pagesFlagging and Result Interpretation-1Rini WidyantariNo ratings yet
- Presentation Hematology Analyzer SAM MedanDocument135 pagesPresentation Hematology Analyzer SAM MedanJeffry NugrahaNo ratings yet
- Tumor Markeri - Eng PDFDocument79 pagesTumor Markeri - Eng PDFdr_4uNo ratings yet
- 1.1 Bacterial Morphology Structure and ClassificationDocument108 pages1.1 Bacterial Morphology Structure and ClassificationJustine Mel Concepcion IlardeNo ratings yet
- Immature Platelet Fraction (IPF)Document5 pagesImmature Platelet Fraction (IPF)asankandessNo ratings yet
- Acinetobacter BaumanniiDocument53 pagesAcinetobacter BaumanniiLaboratorium BorromeusNo ratings yet
- Malaria Rapid Diagnostic Test Performance: Results of Who Product Testing of Malaria RDTS: Round 7 (2015-2016)Document164 pagesMalaria Rapid Diagnostic Test Performance: Results of Who Product Testing of Malaria RDTS: Round 7 (2015-2016)clive.mascarenhas909No ratings yet
- Thermal Analysis V2: Inorganic Materials and Physical ChemistryFrom EverandThermal Analysis V2: Inorganic Materials and Physical ChemistryRobert F. Jr. SchwenkerRating: 1 out of 5 stars1/5 (1)
- Le Fort 1 Osteotomy and Bilateral Sagittal Split Osteotomy (Bsso) For Treatment of Mandibular Prognathism and Maxillary RetrusionDocument13 pagesLe Fort 1 Osteotomy and Bilateral Sagittal Split Osteotomy (Bsso) For Treatment of Mandibular Prognathism and Maxillary RetrusionJenadi BinartoNo ratings yet
- 10 1016@j Rmo 2016 03 068 PDFDocument9 pages10 1016@j Rmo 2016 03 068 PDFJenadi BinartoNo ratings yet
- JournalDocument1 pageJournalJenadi BinartoNo ratings yet
- SSC BundleDocument2 pagesSSC BundleFrancisco MañánNo ratings yet
- Taat11i1sjip20 PDFDocument10 pagesTaat11i1sjip20 PDFJenadi BinartoNo ratings yet
- Tatullo Et Al-2014-Journal of Tissue Engineering and Regenerative MedicineDocument12 pagesTatullo Et Al-2014-Journal of Tissue Engineering and Regenerative MedicineJenadi BinartoNo ratings yet
- 6 ACasereportDocument7 pages6 ACasereportJenadi BinartoNo ratings yet
- Head Trauma: Kelompok 2: Andry Wongso Rhiza M.I.S Terri S. S PriscillaDocument22 pagesHead Trauma: Kelompok 2: Andry Wongso Rhiza M.I.S Terri S. S PriscillaJenadi BinartoNo ratings yet
- Immunology 3Document66 pagesImmunology 3Denise JohnsonNo ratings yet
- Detect blood, parasites and nutritional content in stoolDocument11 pagesDetect blood, parasites and nutritional content in stoolJenadi BinartoNo ratings yet
- 1720 5516 1 PBDocument4 pages1720 5516 1 PBJenadi BinartoNo ratings yet
- 2003 Lab Ev. in DMDocument2 pages2003 Lab Ev. in DMJenadi BinartoNo ratings yet
- Renal FunctionDocument28 pagesRenal FunctionJenadi BinartoNo ratings yet
- Head Trauma: Kelompok 2: Andry Wongso Rhiza M.I.S Terri S. S PriscillaDocument22 pagesHead Trauma: Kelompok 2: Andry Wongso Rhiza M.I.S Terri S. S PriscillaJenadi BinartoNo ratings yet
- AlveOlar June July 09Document2 pagesAlveOlar June July 09Jenadi BinartoNo ratings yet
- Transfusi Darah dan PermasalahannyaDocument142 pagesTransfusi Darah dan PermasalahannyaJenadi BinartoNo ratings yet
- GERDDocument11 pagesGERDJenadi BinartoNo ratings yet
- Use of 3-D Stereolithographic Models in Oral and Maxillofacial SurgeryDocument8 pagesUse of 3-D Stereolithographic Models in Oral and Maxillofacial SurgeryJenadi BinartoNo ratings yet
- Over View of BloodDocument42 pagesOver View of BloodJenadi BinartoNo ratings yet
- Hepatitis Virus KuliahDocument54 pagesHepatitis Virus KuliahJenadi BinartoNo ratings yet
- Hegewald Et Al-2013-Journal of Tissue Engineering and Regenerative MedicineDocument10 pagesHegewald Et Al-2013-Journal of Tissue Engineering and Regenerative MedicineJenadi BinartoNo ratings yet
- Anemia & Leukemia PKDocument35 pagesAnemia & Leukemia PKJenadi BinartoNo ratings yet
- Aids - FKGDocument74 pagesAids - FKGJenadi BinartoNo ratings yet
- Over View of BloodDocument42 pagesOver View of BloodJenadi BinartoNo ratings yet
- Pathophysiology of Laboratory Abnormalities in Liver DisordersDocument55 pagesPathophysiology of Laboratory Abnormalities in Liver DisordersYudha fedrian AKNo ratings yet
- DownloadDocument10 pagesDownloadhasan nazzalNo ratings yet
- CBCT Imaging in TMDDocument11 pagesCBCT Imaging in TMDJenadi BinartoNo ratings yet
- Use of 3-D Stereolithographic Models in Oral and Maxillofacial SurgeryDocument8 pagesUse of 3-D Stereolithographic Models in Oral and Maxillofacial SurgeryJenadi BinartoNo ratings yet
- AKI in TraumaDocument13 pagesAKI in TraumaJenadi BinartoNo ratings yet
- Urine Albumin NewDocument10 pagesUrine Albumin NewPriya Sharma100% (1)
- Dengue Clinical Presentation - History, Physical ExaminationDocument6 pagesDengue Clinical Presentation - History, Physical Examinationm.m.m.mNo ratings yet
- Hipokalemia: KaliumDocument49 pagesHipokalemia: KaliumIqbalAmriFauzalNo ratings yet
- Pol TakesDocument84 pagesPol Takesfauzi jayaNo ratings yet
- Aortic ValveDocument8 pagesAortic ValveIfeanyichukwu OgbonnayaNo ratings yet
- The effects of tobacco use on oral healthDocument8 pagesThe effects of tobacco use on oral healthRivandy HolilNo ratings yet
- Update on Lower Lid Blepharoplasty TechniquesDocument23 pagesUpdate on Lower Lid Blepharoplasty TechniquesNur baitiNo ratings yet
- Health Declaration Health Declaration: City of Mati City of MatiDocument2 pagesHealth Declaration Health Declaration: City of Mati City of MatiHannah Marie AlbeteNo ratings yet
- ArthropodaDocument36 pagesArthropodatapas kunduNo ratings yet
- Blood Agar Base (Infusion Agar) : Intended Use Summary and ExplanationDocument2 pagesBlood Agar Base (Infusion Agar) : Intended Use Summary and ExplanationSarehElizabetNo ratings yet
- Universal Credit Work Capability QuestionnaireDocument24 pagesUniversal Credit Work Capability QuestionnaireSteven Preece100% (2)
- Rhinitis: Sheryl BeardDocument14 pagesRhinitis: Sheryl BeardJohar TajudinNo ratings yet
- Nervous System Infections GuideDocument91 pagesNervous System Infections GuideBea Bianca CruzNo ratings yet
- Certificate of Accreditation: Swift Silliker (Pty) LTDDocument10 pagesCertificate of Accreditation: Swift Silliker (Pty) LTDpham xuan tinh tinhNo ratings yet
- Parameters of Mechanics of BreathingDocument16 pagesParameters of Mechanics of BreathingKaioNo ratings yet
- Recent Advances in Sensing Plant Diseases For Precision Crop Protection PDFDocument13 pagesRecent Advances in Sensing Plant Diseases For Precision Crop Protection PDFJhon ReyesNo ratings yet
- Drug StudyDocument4 pagesDrug StudyJessica GlitterNo ratings yet
- Seizures and The Epilepsies in Infants, Children, and AdolescentsDocument8 pagesSeizures and The Epilepsies in Infants, Children, and AdolescentsCecille Ann CayetanoNo ratings yet
- Ls Models Top 100 Preteen Models Non NudeDocument2 pagesLs Models Top 100 Preteen Models Non NudeFrancisco Lima de SousaNo ratings yet
- FirstAid 2017 PDFDocument412 pagesFirstAid 2017 PDFSylvia Diamond86% (7)
- Vol. 2 No. 10Document58 pagesVol. 2 No. 10Lindsey RobbinsNo ratings yet
- Difficult Decissions in TraumaDocument443 pagesDifficult Decissions in Traumajulio vilela100% (1)
- Full Download High Acuity Nursing 6th Edition Wagner Test BankDocument18 pagesFull Download High Acuity Nursing 6th Edition Wagner Test Bankassapancopepodmhup100% (38)
- Medical Surgical NursingDocument38 pagesMedical Surgical NursingTripti PunNo ratings yet
- CytologyDocument12 pagesCytologyEsther HutagalungNo ratings yet
- British Orthoptic Journal 2002Document9 pagesBritish Orthoptic Journal 2002roelkloosNo ratings yet
- YMMNO ProposalDocument2 pagesYMMNO ProposalYamon Min Nyunt OoNo ratings yet
- Comprehensive Textbook of SurgeryDocument338 pagesComprehensive Textbook of SurgeryAdel Saleh100% (1)
- q004 Little A Little Few A Few PDFDocument2 pagesq004 Little A Little Few A Few PDFmabel alicia marcial0% (1)
- Clinical Manifestations and Management of Hospitalized Women With Bartholin Versus Non Bartholin Vulvar AbscessDocument4 pagesClinical Manifestations and Management of Hospitalized Women With Bartholin Versus Non Bartholin Vulvar AbscessPaul HartingNo ratings yet