You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
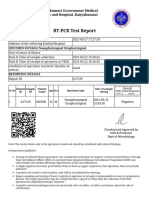
- RT-PCR Test Report: Kanyakumari Government Medical College and Hospital, KanyakumariDocument2 pagesRT-PCR Test Report: Kanyakumari Government Medical College and Hospital, KanyakumariAnithaNo ratings yet
- Test Result Normal Range Interpreta Tion Implicatio NDocument11 pagesTest Result Normal Range Interpreta Tion Implicatio NSitty Aizah MangotaraNo ratings yet
- Pagos Efectuados A LaboratoriosDocument14 pagesPagos Efectuados A LaboratoriosCronista.comNo ratings yet
- CDC 1st Quar. REPORT 2015Document67 pagesCDC 1st Quar. REPORT 2015abdi qanoNo ratings yet
- JKN Ketentuan RanapDocument8 pagesJKN Ketentuan RanapIkeNo ratings yet
- COVID-19 consumable products catalogDocument2 pagesCOVID-19 consumable products catalogRadit AMSNo ratings yet
- 080001Document21 pages080001Pearl MayNo ratings yet
- Conjunctivitis, Eye (Conjunctivitis), Pink EyeDocument1 pageConjunctivitis, Eye (Conjunctivitis), Pink EyeTudorel PoalelungiNo ratings yet
- Science As Human Endeavour TaskDocument2 pagesScience As Human Endeavour Taskyolanda Sitepu100% (1)
- Eye infection prevalence and patient profiles at Manado Eye HospitalDocument5 pagesEye infection prevalence and patient profiles at Manado Eye HospitalDarwin ThenNo ratings yet
- LabReportNew - 2023-06-23T171149.608Document1 pageLabReportNew - 2023-06-23T171149.608B AZAD SIMHANo ratings yet
- Rounds: Case Study and Review of Autoimmune HepatitisDocument7 pagesRounds: Case Study and Review of Autoimmune HepatitisClaudia Naomi Ventura OrtizNo ratings yet
- Revision For BioDocument7 pagesRevision For BioJustt MeeNo ratings yet
- Blood Components: Red CellsDocument4 pagesBlood Components: Red CellsKyle Ambis SyNo ratings yet
- About Tattoos What Is A Tattoo?Document2 pagesAbout Tattoos What Is A Tattoo?Çağatay SarıkayaNo ratings yet
- Pemphigus GuideDocument8 pagesPemphigus Guidezuqiri ChanelNo ratings yet
- Precipitation and Agglutination ReactionsDocument3 pagesPrecipitation and Agglutination ReactionsakiNo ratings yet
- IB Biology Topic 11 - Animal Physiology HL Revision SheetDocument1 pageIB Biology Topic 11 - Animal Physiology HL Revision SheetLexieNo ratings yet
- Blood: Muhammad Iqbal Lecturer KMUDocument40 pagesBlood: Muhammad Iqbal Lecturer KMUKomal NayabNo ratings yet
- COVID-19 Source Book: Third EditionDocument64 pagesCOVID-19 Source Book: Third EditionNikolaos GonosNo ratings yet
- Depo Medrol 80 MG - Google SearchDocument1 pageDepo Medrol 80 MG - Google SearchMohammad AamirNo ratings yet
- Infectious Mono Signs, Symptoms, and PreventionDocument3 pagesInfectious Mono Signs, Symptoms, and PreventionJAN ELMER L. LABESORESNo ratings yet
- BronchioitisDocument24 pagesBronchioitismitiku aberaNo ratings yet
- Presentasi Jurnal Besar - 31may 2020 FIXDocument38 pagesPresentasi Jurnal Besar - 31may 2020 FIXEka HerlinggaNo ratings yet
- BB Lab MidtermDocument3 pagesBB Lab MidtermYo Issei HyodonoNo ratings yet
- Bacteria PDFDocument13 pagesBacteria PDFJohn Christopher LucesNo ratings yet
- Principles of Immunodetection 2Document59 pagesPrinciples of Immunodetection 2Martha RetnaningtyasNo ratings yet
- Antigen Presenting CellDocument26 pagesAntigen Presenting CellSurja DasNo ratings yet
- DM 2020-0351 HPVDocument9 pagesDM 2020-0351 HPVShardin Labawan-Juen,RNNo ratings yet
- MeningitisDocument12 pagesMeningitisFaith Vaughn100% (2)