You might also like
- Eiji Yoshikawa - Musashi 1 EarthDocument78 pagesEiji Yoshikawa - Musashi 1 EarthaerapianginNo ratings yet
- Rheumatoid ArthritisDocument2 pagesRheumatoid ArthritisAri Puji AstutiNo ratings yet
- A Review On Anti-Tubercular PlantsDocument9 pagesA Review On Anti-Tubercular PlantsAri Puji AstutiNo ratings yet
- Terpenoid FriedelinDocument4 pagesTerpenoid FriedelinAri Puji Astuti100% (1)
- Terpenoid FriedelinDocument4 pagesTerpenoid FriedelinAri Puji Astuti100% (1)
- Antiviral FarmasiDocument46 pagesAntiviral FarmasiAri Puji AstutiNo ratings yet
- 060 JimenezDocument6 pages060 JimenezAri Puji AstutiNo ratings yet
- Sesquiterpene Lactones - Structural Diversity and Their Biological ActivitiesDocument22 pagesSesquiterpene Lactones - Structural Diversity and Their Biological ActivitiesAri Puji AstutiNo ratings yet
- Anestesi Umum Dan LokalDocument34 pagesAnestesi Umum Dan LokalAri Puji Astuti100% (1)
- Muscle RelaxantDocument29 pagesMuscle RelaxantAri Puji AstutiNo ratings yet
- StabiloDocument6 pagesStabiloAri Puji AstutiNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Sop EcuDocument11 pagesSop Ecuahmed saeedNo ratings yet
- Emperger's pioneering composite columnsDocument11 pagesEmperger's pioneering composite columnsDishant PrajapatiNo ratings yet
- Chapter 7 - Cash BudgetDocument23 pagesChapter 7 - Cash BudgetMostafa KaghaNo ratings yet
- Backup and Recovery ScenariosDocument8 pagesBackup and Recovery ScenariosAmit JhaNo ratings yet
- Customer Satisfaction and Brand Loyalty in Big BasketDocument73 pagesCustomer Satisfaction and Brand Loyalty in Big BasketUpadhayayAnkurNo ratings yet
- ABBBADocument151 pagesABBBAJeremy MaraveNo ratings yet
- SAP ORC Opportunities PDFDocument1 pageSAP ORC Opportunities PDFdevil_3565No ratings yet
- An4856 Stevalisa172v2 2 KW Fully Digital Ac DC Power Supply Dsmps Evaluation Board StmicroelectronicsDocument74 pagesAn4856 Stevalisa172v2 2 KW Fully Digital Ac DC Power Supply Dsmps Evaluation Board StmicroelectronicsStefano SalaNo ratings yet
- Qatar Airways E-ticket Receipt for Travel from Baghdad to AthensDocument1 pageQatar Airways E-ticket Receipt for Travel from Baghdad to Athensمحمد الشريفي mohammed alshareefiNo ratings yet
- SyllabusDocument4 pagesSyllabusapi-105955784No ratings yet
- Prestressing ProductsDocument40 pagesPrestressing ProductsSakshi Sana100% (1)
- BS EN 364-1993 (Testing Methods For Protective Equipment AgaiDocument21 pagesBS EN 364-1993 (Testing Methods For Protective Equipment AgaiSakib AyubNo ratings yet
- SE Myth of SoftwareDocument3 pagesSE Myth of SoftwarePrakash PaudelNo ratings yet
- 3DS MAX SYLLABUSDocument8 pages3DS MAX SYLLABUSKannan RajaNo ratings yet
- Haryana Retial GarmentsDocument8 pagesHaryana Retial Garmentssudesh.samastNo ratings yet
- Ju Complete Face Recovery GAN Unsupervised Joint Face Rotation and De-Occlusion WACV 2022 PaperDocument11 pagesJu Complete Face Recovery GAN Unsupervised Joint Face Rotation and De-Occlusion WACV 2022 PaperBiponjot KaurNo ratings yet
- Information Pack For Indonesian Candidate 23.06.2023Document6 pagesInformation Pack For Indonesian Candidate 23.06.2023Serevinna DewitaNo ratings yet
- 5.PassLeader 210-260 Exam Dumps (121-150)Document9 pages5.PassLeader 210-260 Exam Dumps (121-150)Shaleh SenNo ratings yet
- Corruption in PakistanDocument15 pagesCorruption in PakistanklutzymeNo ratings yet
- Sample Property Management AgreementDocument13 pagesSample Property Management AgreementSarah TNo ratings yet
- SDNY - Girl Scouts V Boy Scouts ComplaintDocument50 pagesSDNY - Girl Scouts V Boy Scouts Complaintjan.wolfe5356No ratings yet
- Tutorial 5 HExDocument16 pagesTutorial 5 HExishita.brahmbhattNo ratings yet
- Programme Report Light The SparkDocument17 pagesProgramme Report Light The SparkAbhishek Mishra100% (1)
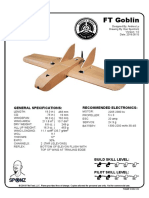
- FT Goblin Full SizeDocument7 pagesFT Goblin Full SizeDeakon Frost100% (1)
- Model S-20 High Performance Pressure Transmitter For General Industrial ApplicationsDocument15 pagesModel S-20 High Performance Pressure Transmitter For General Industrial ApplicationsIndra PutraNo ratings yet
- Sav 5446Document21 pagesSav 5446Michael100% (2)
- Green Management: Nestlé's Approach To Green Management 1. Research and DevelopmentDocument6 pagesGreen Management: Nestlé's Approach To Green Management 1. Research and DevelopmentAbaidullah TanveerNo ratings yet
- Proposed Delivery For PAU/AHU Method Statement SEC/MS/3-25Document4 pagesProposed Delivery For PAU/AHU Method Statement SEC/MS/3-25Zin Ko NaingNo ratings yet
- New Installation Procedures - 2Document156 pagesNew Installation Procedures - 2w00kkk100% (2)
- Theme Meal ReportDocument10 pagesTheme Meal Reportapi-434982019No ratings yet