You might also like
- EarthDocument1 pageEarthMica SaeronNo ratings yet
- CephalosporinsDocument25 pagesCephalosporinsBubulax2No ratings yet
- Kim 3Document1 pageKim 3Mica SaeronNo ratings yet
- HoyDocument1 pageHoyMica SaeronNo ratings yet
- Blood ComponenteDocument1 pageBlood ComponenteMica SaeronNo ratings yet
- FUJIFILM NX500 DRI CHEM Brochure - 1Document2 pagesFUJIFILM NX500 DRI CHEM Brochure - 1Alyssa Sagario100% (1)
- The Announcement of JohnDocument2 pagesThe Announcement of JohnMica SaeronNo ratings yet
- LoveDocument1 pageLoveMica SaeronNo ratings yet
- Wa 5 CHDocument1 pageWa 5 CHMica SaeronNo ratings yet
- I Love YouDocument1 pageI Love YouMica SaeronNo ratings yet
- God Is Good All The TimeDocument1 pageGod Is Good All The TimeMica SaeronNo ratings yet
- Compare Amd ContrastDocument1 pageCompare Amd ContrastMica SaeronNo ratings yet
- Meanig LessDocument1 pageMeanig LessMica SaeronNo ratings yet
- Practical MicrobiologyDocument1 pagePractical MicrobiologyMica SaeronNo ratings yet
- Executive Order No 12Document5 pagesExecutive Order No 12Mica SaeronNo ratings yet
- Publish To The WorldDocument1 pagePublish To The WorldMica SaeronNo ratings yet
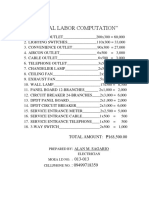
- Electrical Labor ComputationDocument2 pagesElectrical Labor ComputationMica SaeronNo ratings yet
- AdfdffgmkjfmcsdkmfdDocument1 pageAdfdffgmkjfmcsdkmfdMica SaeronNo ratings yet
- CV-polar Flagella PE - Multiple Flagella: Spore Survives in BC GRAM POS OBLIGATE AEROBE - Bacillus, NocardiaDocument4 pagesCV-polar Flagella PE - Multiple Flagella: Spore Survives in BC GRAM POS OBLIGATE AEROBE - Bacillus, NocardiaMica SaeronNo ratings yet
- Lord Lord Lord Lord LordDocument1 pageLord Lord Lord Lord LordMica SaeronNo ratings yet
- Compare Amd ContrastDocument1 pageCompare Amd ContrastMica SaeronNo ratings yet
- What Do You Mean, Not Based On My Suspicions Alone?: The Literature ReviewDocument2 pagesWhat Do You Mean, Not Based On My Suspicions Alone?: The Literature ReviewMica SaeronNo ratings yet
- Compare Amd ContrastDocument1 pageCompare Amd ContrastMica SaeronNo ratings yet
- Lord Lord Lord Lord LordDocument1 pageLord Lord Lord Lord LordMica SaeronNo ratings yet
- List of Teenage PregnancyDocument1 pageList of Teenage PregnancyMica SaeronNo ratings yet
- BeautifulDocument2 pagesBeautifulMica SaeronNo ratings yet
- Name: Khea Fernandez Grade/Strand: G-11 ABM 4Document1 pageName: Khea Fernandez Grade/Strand: G-11 ABM 4Mica SaeronNo ratings yet
- FlowerDocument2 pagesFlowerMica SaeronNo ratings yet
- True FriendDocument3 pagesTrue FriendMica SaeronNo ratings yet
- AloneDocument2 pagesAloneMica SaeronNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Second Summative TestDocument2 pagesSecond Summative TestEthel Wenceslao100% (2)
- Renal Ultrasound BMUS Study Day: Rosie ConlonDocument72 pagesRenal Ultrasound BMUS Study Day: Rosie ConlonlllorellleiNo ratings yet
- The Essential Review Guide For Passing The Mblex Licensing Exam 2017 EditionDocument192 pagesThe Essential Review Guide For Passing The Mblex Licensing Exam 2017 EditionSabrina Marie100% (3)
- Anatomia Dezvoltarii PancreasuluiDocument49 pagesAnatomia Dezvoltarii Pancreasuluitarra abuNo ratings yet
- Dr. YSR Aarogyasri Health Care TrustDocument23 pagesDr. YSR Aarogyasri Health Care Trusttatapudi mohanNo ratings yet
- Block Hepatobiliary SystemDocument29 pagesBlock Hepatobiliary SystemKevin KusumanNo ratings yet
- Office of The Provincial ProsecutorDocument15 pagesOffice of The Provincial ProsecutorKenneth CabesNo ratings yet
- Glandular EpitheliumDocument5 pagesGlandular EpitheliumNakuru SandwichNo ratings yet
- Blood TypingDocument2 pagesBlood TypingEnaye MajiriNo ratings yet
- Body Parts/ System & Method of Assessment Used Actual Findings Normal Findings InterpretationDocument8 pagesBody Parts/ System & Method of Assessment Used Actual Findings Normal Findings InterpretationMack Javier VenturaNo ratings yet
- Seminal Fluid Analysis: Purpose of The TestDocument13 pagesSeminal Fluid Analysis: Purpose of The TestChristian Morfe MacdonNo ratings yet
- Nonextraction Treatment of An Adult With Class Ii Division 2 MalocclusionDocument9 pagesNonextraction Treatment of An Adult With Class Ii Division 2 MalocclusionDrManem Jaganath VenkatNo ratings yet
- Histology of GitDocument31 pagesHistology of GitLucky LuckyNo ratings yet
- Anatomy of The Rectum and Anal Canal: The Rectum Is The Part of The Colon Between The Sigmoid ColonDocument25 pagesAnatomy of The Rectum and Anal Canal: The Rectum Is The Part of The Colon Between The Sigmoid ColonJoy GhoseNo ratings yet
- Dental Record FormDocument1 pageDental Record FormadoptifyNo ratings yet
- Medical Surgical Nursing OrthopedicDocument22 pagesMedical Surgical Nursing Orthopedicroger80% (5)
- Spine Lesson PlanDocument5 pagesSpine Lesson Planapi-37914933950% (2)
- Lecture Notes in Medical Technology - Lecture #5 - THYROID FUNCTION TESTSDocument14 pagesLecture Notes in Medical Technology - Lecture #5 - THYROID FUNCTION TESTSKat JornadalNo ratings yet
- Human Reproduction WorksheetDocument3 pagesHuman Reproduction WorksheetDEEBAN0% (1)
- Hemodynamic Disorders Thromboembolic Disease and ShockDocument13 pagesHemodynamic Disorders Thromboembolic Disease and ShockAbu HuraraNo ratings yet
- NeuroDocument35 pagesNeuroFlor OMNo ratings yet
- NJ Dolphin Necropsy ReportDocument5 pagesNJ Dolphin Necropsy ReportopracrusadesNo ratings yet
- Complete Eloptic Directory (OCR) PDFDocument308 pagesComplete Eloptic Directory (OCR) PDFAnonymous SCZ4uYNo ratings yet
- Tugas Bahasa InggrisDocument2 pagesTugas Bahasa InggrisrikaNo ratings yet
- The Female Reproductive System: Dr. Emanuel Muro HkmuDocument41 pagesThe Female Reproductive System: Dr. Emanuel Muro HkmuMustafa DadahNo ratings yet
- 002 Handout Basic Concepts Part 2Document8 pages002 Handout Basic Concepts Part 2Alfred BajarNo ratings yet
- Brain Hat StepsDocument2 pagesBrain Hat StepsPsic. Ó. Bernardo Duarte B.No ratings yet
- 1.case Presentation CHDDocument23 pages1.case Presentation CHDDHARM MEENA0% (1)
- Sophia Solanilla 7°U Classwork #3 The Circulatory SystemDocument3 pagesSophia Solanilla 7°U Classwork #3 The Circulatory SystemSOPHIA TIMENo ratings yet
- MRCS A Paper 1 SBAs Applied Basic Sci 2eDocument17 pagesMRCS A Paper 1 SBAs Applied Basic Sci 2eaeages100% (1)