You might also like
- Pulmonary EmbolismDocument16 pagesPulmonary EmbolismEhab Mokhtar WehebaNo ratings yet
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Pulmonary EmbolismDocument23 pagesPulmonary EmbolismBianca Dizon0% (1)
- A Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Hypertrophic Cardiomyopathy: Board Review Rami Khouzam, MDDocument89 pagesHypertrophic Cardiomyopathy: Board Review Rami Khouzam, MDmsmith6477No ratings yet
- Mitral StenosisDocument17 pagesMitral StenosisMuhammad Alauddin Sarwar100% (8)
- Hypertrophic CardiomyopathyDocument57 pagesHypertrophic CardiomyopathycynNo ratings yet
- PneumothoraxDocument52 pagesPneumothoraxtrisna satrianaNo ratings yet
- Pulmonary EmbolismDocument96 pagesPulmonary Embolismsamice5100% (1)
- 10 CardiomyopathyDocument71 pages10 CardiomyopathyAnonymous vUEDx8100% (5)
- Cardiogenic Shock PDFDocument14 pagesCardiogenic Shock PDFAdreiTheTripleANo ratings yet
- Mitral Stenosis PresentationDocument84 pagesMitral Stenosis PresentationStawan Chougule100% (2)
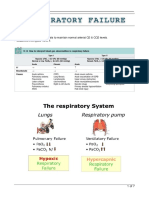
- Respiratory FailureDocument7 pagesRespiratory FailureLulu100% (1)
- Pulmonary EdemaDocument59 pagesPulmonary EdemamaibejoseNo ratings yet
- Infective Endocarditis: Christine Joy F. Baquiran MED-3CDocument46 pagesInfective Endocarditis: Christine Joy F. Baquiran MED-3CAbigail SabinoNo ratings yet
- Cor PulmonaleDocument62 pagesCor PulmonaleAlbert NixonNo ratings yet
- Pulmonaryembolism 150329161109 Conversion Gate01Document60 pagesPulmonaryembolism 150329161109 Conversion Gate01Rafika RaraNo ratings yet
- Assessment of Right Ventricular FunctionDocument41 pagesAssessment of Right Ventricular FunctionAditya MadhavpeddiNo ratings yet
- Cardiomyopathy and Myocarditis HarrisonsDocument62 pagesCardiomyopathy and Myocarditis HarrisonsGrace CastilloNo ratings yet
- Acute Coronary SyndromeDocument21 pagesAcute Coronary SyndromeNabil Mosharraf Hossain100% (2)
- Cor Pulmonale: Dr. Gerrard UyDocument13 pagesCor Pulmonale: Dr. Gerrard Uyfaridah azzah sariNo ratings yet
- Chest Tube ManagementDocument27 pagesChest Tube ManagementIanne Merh100% (2)
- Atrial FibrillationDocument35 pagesAtrial FibrillationKABERA RENE100% (2)
- Cardiac TamponadeDocument10 pagesCardiac TamponadeRahmi Fatma SariNo ratings yet
- ARDSDocument82 pagesARDSfeniNo ratings yet
- Tutorial in ECG: Dr. Chew Keng Sheng Emergency Medicine Universiti Sains MalaysiaDocument56 pagesTutorial in ECG: Dr. Chew Keng Sheng Emergency Medicine Universiti Sains Malaysiafeby_valNo ratings yet
- Heart Failure in ChildrenDocument44 pagesHeart Failure in ChildrenRisna Ariani100% (2)
- CardiomyopathyDocument19 pagesCardiomyopathyAhmad AgielNo ratings yet
- Assessment of The Critically Ill PatientDocument5 pagesAssessment of The Critically Ill PatientCris John RicoNo ratings yet
- Tension Pneumothorax 170102133730Document21 pagesTension Pneumothorax 170102133730novelraaaNo ratings yet
- Dilated CardiomyopathyDocument13 pagesDilated CardiomyopathyPrincysuzine PintoNo ratings yet
- Pulmonary EmbolismDocument14 pagesPulmonary EmbolismAngel Naypes ReyesNo ratings yet
- Pulmonary EmbolismDocument21 pagesPulmonary EmbolismMadhu Bala100% (2)
- Pneumonectomy S RT RpaDocument4 pagesPneumonectomy S RT RpagireeshsachinNo ratings yet
- Pulmonary HypertensionDocument35 pagesPulmonary HypertensionKea Keleste DetablanNo ratings yet
- Presentation Chapter 27 Pulmonary Embolism and ARDS CaseDocument91 pagesPresentation Chapter 27 Pulmonary Embolism and ARDS Caseavoyiad100% (1)
- Cyanotic Congenital Heart DiseaseDocument80 pagesCyanotic Congenital Heart DiseaseJessica StephanieNo ratings yet
- 5 MED 4 - Approach To GI BleedingDocument6 pages5 MED 4 - Approach To GI BleedingIan CruzNo ratings yet
- CHF, HPN and CAPDocument17 pagesCHF, HPN and CAPJhune VillegasNo ratings yet
- Atrial Fibrillation (AF)Document24 pagesAtrial Fibrillation (AF)farmasi_hm100% (1)
- Acute Resp FailureDocument52 pagesAcute Resp FailureAlex ChiuNo ratings yet
- Right Ventricular Myocardial InfarctionDocument43 pagesRight Ventricular Myocardial Infarctionrudresh m g0% (2)
- Rheumatic Heart Disease AustrliaDocument63 pagesRheumatic Heart Disease AustrliaMuhammad Reza100% (2)
- Liver Anatomy and Physiology MedicineDocument73 pagesLiver Anatomy and Physiology MedicineRobin TolentinoNo ratings yet
- Acute Respiratory Distress SyndromeDocument70 pagesAcute Respiratory Distress SyndromeAndrea Del Villar100% (1)
- Pulmonary EmbolismDocument8 pagesPulmonary EmbolismspoilttbrattNo ratings yet
- Mitral Stenosis Mitral RegurgitationDocument66 pagesMitral Stenosis Mitral RegurgitationMarshellaTriPradilagaNo ratings yet
- Bronchial AsthmaDocument27 pagesBronchial AsthmachandrikaismailNo ratings yet
- 13.acute Respiratory FailureDocument34 pages13.acute Respiratory Failurekarim hassan100% (1)
- Congenital Heart DiseaseDocument124 pagesCongenital Heart DiseasemulkanmustafaNo ratings yet
- Cardiac AsthmaDocument12 pagesCardiac AsthmaNeupane KsabNo ratings yet
- Mitral StenosisDocument43 pagesMitral StenosisEricka SantosNo ratings yet
- Infective EndocarditisDocument18 pagesInfective EndocarditisSam100% (1)
- Hypovolemic Shock TEXTDocument5 pagesHypovolemic Shock TEXTrhen1991No ratings yet
- Acute Respiratory Distress SyndromeDocument36 pagesAcute Respiratory Distress Syndromedr9348345000No ratings yet
- Management of Infective EndocarditisDocument14 pagesManagement of Infective Endocarditismhafzam2020No ratings yet
- Right Sided Heart FailureDocument33 pagesRight Sided Heart FailurePaulNo ratings yet
- Pulmonary EmbolismDocument5 pagesPulmonary EmbolismNica Duco100% (2)
- Cardiomyopathy: Dr. Ibrahim AbuasbehDocument39 pagesCardiomyopathy: Dr. Ibrahim Abuasbehأبوأحمد الحكيمNo ratings yet
- Jugular Venous Pressure: It's Easier Than It LooksDocument25 pagesJugular Venous Pressure: It's Easier Than It LooksManggarsari SdwqNo ratings yet
- DORVDocument5 pagesDORVkelly christyNo ratings yet
- American Journal of Emergency Medicine: J. Rabjohns, T. Quan, K. Boniface, A. PourmandDocument5 pagesAmerican Journal of Emergency Medicine: J. Rabjohns, T. Quan, K. Boniface, A. Pourmandmaria Luisa VillaseñorNo ratings yet
- EKG Quick and Dirty - GD v3.0Document2 pagesEKG Quick and Dirty - GD v3.0Sheema Sh100% (1)
- Holter Monitoring: Dr. Kazi Alam NowazDocument19 pagesHolter Monitoring: Dr. Kazi Alam NowazRadison sierraNo ratings yet
- VT Origin PDFDocument60 pagesVT Origin PDFNikita PratamaNo ratings yet
- Ic Interactive Product Catalogue Uk 2017Document83 pagesIc Interactive Product Catalogue Uk 2017RABAH BOUCHELAGHEMNo ratings yet
- Cardiac DiseasesDocument8 pagesCardiac DiseasesTJ NgNo ratings yet
- Basic Arrythmia AnalysisDocument60 pagesBasic Arrythmia AnalysisZakky KurniawanNo ratings yet
- Jurnal 4 Uji Jalan 6 MenitDocument10 pagesJurnal 4 Uji Jalan 6 MenitSandy Tama Okvan YudhaNo ratings yet
- Aritmia Dan Kardiotonik Eng UciDocument36 pagesAritmia Dan Kardiotonik Eng UciUci RamadhantyNo ratings yet
- Board 14 Desember 2014 Kumpulan FinalDocument73 pagesBoard 14 Desember 2014 Kumpulan FinalAnonymous XHguqDfWR0% (1)
- Basic Arrhythmia RulesDocument3 pagesBasic Arrhythmia Rulesgreenflames0997% (30)
- WP202208-HeartAssistTM For AdultDocument20 pagesWP202208-HeartAssistTM For AdultAlan BiNo ratings yet
- Rate and RhythmDocument10 pagesRate and RhythmSamanta Luiza de AraujoNo ratings yet
- Cardio Script OSCEDocument2 pagesCardio Script OSCEbarb gNo ratings yet
- Gambro Phoenix SystemDocument2 pagesGambro Phoenix SystemGraham Thomas GipsonNo ratings yet
- Sudden Cardiac Death: Ischaemic Heart DiseaseDocument4 pagesSudden Cardiac Death: Ischaemic Heart Diseasenmyza89No ratings yet
- Glomerular DiseasesDocument16 pagesGlomerular DiseasesSamuel kuriaNo ratings yet
- Draw Cardiac Arrest Algorithm (Aha)Document21 pagesDraw Cardiac Arrest Algorithm (Aha)Thanyun YunNo ratings yet
- Atrial FibrillationDocument19 pagesAtrial FibrillationAnwari MuhammadNo ratings yet
- Renal FailureDocument23 pagesRenal FailurerjfeeleyNo ratings yet
- Critical Care Medicine Certification Examination Blueprint - American Board of Internal MedicineDocument6 pagesCritical Care Medicine Certification Examination Blueprint - American Board of Internal MedicineabimorgNo ratings yet
- DNB (Post MBBS) January 2017 Admission Session - Seat Allotment Details (Round-1)Document49 pagesDNB (Post MBBS) January 2017 Admission Session - Seat Allotment Details (Round-1)Karan KalraNo ratings yet
- 10introduction To EchocardiographyDocument21 pages10introduction To EchocardiographyMaria EdelNo ratings yet
- IFU Acticor 439128-F EsDocument143 pagesIFU Acticor 439128-F EsMartin ArrietaNo ratings yet
- Resuscitation Training 2016 - KKMDocument60 pagesResuscitation Training 2016 - KKMSiti NabilaNo ratings yet
- CPR Class QuestionnaireDocument4 pagesCPR Class QuestionnaireParikshit PekhaleNo ratings yet
- Pericarditis: Assessment and Diagnostic FindingsDocument3 pagesPericarditis: Assessment and Diagnostic FindingsJANIEZA ANGEL RA�ISES BALTAZARNo ratings yet
- Ventricular Septal DefectDocument18 pagesVentricular Septal DefectJessa Marie AgnesNo ratings yet