You might also like
- Critical Limb IschemiaDocument11 pagesCritical Limb IschemiamohadriaNo ratings yet
- Critical Limb IschemiaDocument11 pagesCritical Limb Ischemianurliah armandNo ratings yet
- Care of Patient With CADDocument22 pagesCare of Patient With CADBader ZawahrehNo ratings yet
- Leriche Fontaine ClassificationDocument8 pagesLeriche Fontaine ClassificationdaxlemonNo ratings yet
- Chronic Venous InsufficiencyDocument29 pagesChronic Venous InsufficiencyariNo ratings yet
- Slide 3: American Heart Association (AHA) in 2016 Stated That 15.5 Million Americans HaveDocument19 pagesSlide 3: American Heart Association (AHA) in 2016 Stated That 15.5 Million Americans HaveChia LengkeyNo ratings yet
- ACS Guide: Acute Coronary Syndrome Definition, Causes, Symptoms & TreatmentDocument2 pagesACS Guide: Acute Coronary Syndrome Definition, Causes, Symptoms & TreatmentRizalNo ratings yet
- Medscape Hypovolemic ShockDocument14 pagesMedscape Hypovolemic ShockSarah Ovinitha100% (1)
- Chronic Critical Limb Ischemia Diagnosis, Treatment and PrognosisDocument14 pagesChronic Critical Limb Ischemia Diagnosis, Treatment and PrognosisHelena A. K. CantikaNo ratings yet
- Acs 1Document65 pagesAcs 1غفران هيثم خليلNo ratings yet
- VASCULITIS SYNDROMESDocument13 pagesVASCULITIS SYNDROMESnitinmaripeddi7No ratings yet
- Shock HypovolemicDocument16 pagesShock HypovolemicTitinNo ratings yet
- Takayasu's Arteritis HHDocument33 pagesTakayasu's Arteritis HHusamadaifallahNo ratings yet
- Angina Pectoris in Patients With A History of Myocardial InfarctionDocument5 pagesAngina Pectoris in Patients With A History of Myocardial Infarctionger4ld1nNo ratings yet
- Pathophysiology and Investigation of Coronary Artery DiseaseDocument4 pagesPathophysiology and Investigation of Coronary Artery DiseasekartikaparamitaNo ratings yet
- Acute Coronary Syndrome (ACS) Pathophysiology and TreatmentDocument39 pagesAcute Coronary Syndrome (ACS) Pathophysiology and TreatmentYowan SusantiNo ratings yet
- Coronary Heart DiseaseDocument23 pagesCoronary Heart DiseaseBEA RADANo ratings yet
- Ischemic Heart DiseaseDocument47 pagesIschemic Heart DiseaseAbood SamoudiNo ratings yet
- Management of Cardiogenic Shock: Clinical UpdateDocument10 pagesManagement of Cardiogenic Shock: Clinical Updateaswad 0008No ratings yet
- Colite IschDocument10 pagesColite IschZakaria QechcharNo ratings yet
- PJT Cvcu Bed 4 Acute Limb IschemicDocument33 pagesPJT Cvcu Bed 4 Acute Limb IschemicHabibie El RamadhaniNo ratings yet
- ONCOLOGICDocument31 pagesONCOLOGICAyessa Yvonne PanganibanNo ratings yet
- Precautions With Diabetic Patients Undergoing SurgeryDocument6 pagesPrecautions With Diabetic Patients Undergoing SurgeryErvin Kyle OsmeñaNo ratings yet
- Shock Cardiogenico - IamDocument19 pagesShock Cardiogenico - IamYESSICA CARENALGANo ratings yet
- Presentation 3Document42 pagesPresentation 3Max ZealNo ratings yet
- Vascular Disease of The BowelDocument28 pagesVascular Disease of The BowelOlga GoryachevaNo ratings yet
- Lec 4Document8 pagesLec 4Sajjad FalahNo ratings yet
- Nicyela Vascular DiseaseDocument21 pagesNicyela Vascular DiseaseNicyela JillienNo ratings yet
- Medically Compromised PatientDocument32 pagesMedically Compromised Patientمحمد عبدالهادي إسماعيلNo ratings yet
- ACS: Acute Coronary SyndromeDocument48 pagesACS: Acute Coronary SyndromeAchmad ulil Albab100% (1)
- CVD DiscussionDocument6 pagesCVD Discussioncataleya mesaNo ratings yet
- Complications of Extremeitiy TraumaDocument11 pagesComplications of Extremeitiy TraumaGilang Kurnia HirawatiNo ratings yet
- Takajasi ArteritisDocument31 pagesTakajasi ArteritisMicija CucuNo ratings yet
- Circulation 2014 Silvain 918 22Document6 pagesCirculation 2014 Silvain 918 22aninNo ratings yet
- Case 5Document16 pagesCase 5Hany ElbarougyNo ratings yet
- 120 Abdominal Compartment SyndromeDocument4 pages120 Abdominal Compartment Syndromewa loneNo ratings yet
- 5 - CABG ModifiedDocument31 pages5 - CABG Modifiedsohilaw210No ratings yet
- Lower Gastrointestinal Bleeding: Practice EssentialsDocument28 pagesLower Gastrointestinal Bleeding: Practice EssentialsJohnPaulOliverosNo ratings yet
- Med Surg Unit 3 Exam ReviewDocument10 pagesMed Surg Unit 3 Exam ReviewIfy OhansonNo ratings yet
- Cardiogenic Shock: Main Causes, Symptoms and TreatmentDocument3 pagesCardiogenic Shock: Main Causes, Symptoms and TreatmentDiaz AlmayangNo ratings yet
- Acute Limb Ischemia - WucDocument37 pagesAcute Limb Ischemia - WucOTOH RAYA OMARNo ratings yet
- Med Surg Assignment 2Document69 pagesMed Surg Assignment 2sham gowliNo ratings yet
- Myocardial InfarctionDocument47 pagesMyocardial Infarctionsanjesh1100% (2)
- Chronic Limb Ischaemic: Dokter Muda: Dedy Sutriyatno Pembinging: Dr. Ivan J. SP - BTKVDocument16 pagesChronic Limb Ischaemic: Dokter Muda: Dedy Sutriyatno Pembinging: Dr. Ivan J. SP - BTKVThe DoctorNo ratings yet
- JAMA Updates On Acute Coronary Syndrome A ReviewDocument13 pagesJAMA Updates On Acute Coronary Syndrome A ReviewRoberto López Mata100% (2)
- Fat Emboli in LiposuctionDocument34 pagesFat Emboli in LiposuctionRicky Herdianto100% (1)
- Advance Concept in Nursing Unit 3Document34 pagesAdvance Concept in Nursing Unit 3Kamran AltafNo ratings yet
- Shock, Arrest, Syncope PhysiopathologyDocument54 pagesShock, Arrest, Syncope PhysiopathologyParsa EbrahimpourNo ratings yet
- Project Injectable Hydrogels as Recent advances in treatment of Myocardial InfarctionDocument16 pagesProject Injectable Hydrogels as Recent advances in treatment of Myocardial Infarctionvarshankpathak2001No ratings yet
- Acute Coronary SyndrommeDocument50 pagesAcute Coronary SyndrommeAndriani Kemala SariNo ratings yet
- Surgical Management of Coronary Artery DiseaseDocument41 pagesSurgical Management of Coronary Artery Diseaseapi-19916399No ratings yet
- Diagnosis and Management of Lower Gastrointestinal Bleeding: Jürgen Barnert and Helmut MessmannDocument10 pagesDiagnosis and Management of Lower Gastrointestinal Bleeding: Jürgen Barnert and Helmut Messmanndwee_RNSNo ratings yet
- Upper Gi Bleed: History, Pe, Pathophysiology, Diagnostics and TreatmentDocument6 pagesUpper Gi Bleed: History, Pe, Pathophysiology, Diagnostics and TreatmentJennicaNo ratings yet
- Coronary Artery Disease and Heart DiseaseDocument37 pagesCoronary Artery Disease and Heart DiseasebtaleraNo ratings yet
- ACS SabistonDocument10 pagesACS Sabistonbocah_britpopNo ratings yet
- Coronary Artery DiseaseDocument22 pagesCoronary Artery DiseaseMamoon RashidNo ratings yet
- Practical Management of Systemic Sclerosis in Clinical PracticeFrom EverandPractical Management of Systemic Sclerosis in Clinical PracticeNo ratings yet
- Unveiling the Unseen: A Journey Into the Hearts Labyrinth SeanFrom EverandUnveiling the Unseen: A Journey Into the Hearts Labyrinth SeanNo ratings yet
- GerdDocument22 pagesGerdAmalia Hendar PangestutiNo ratings yet
- Muntah Dan Obstruksi Saluaran Cerna Atas (I)Document48 pagesMuntah Dan Obstruksi Saluaran Cerna Atas (I)Amalia Hendar PangestutiNo ratings yet
- 3AIDSDocument51 pages3AIDSAmalia Hendar PangestutiNo ratings yet
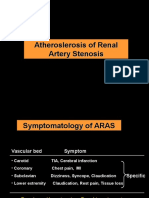
- Symptoms and Treatment of Renal Artery StenosisDocument10 pagesSymptoms and Treatment of Renal Artery StenosisAmalia Hendar PangestutiNo ratings yet
- Fmuntah Dan Obstruksi Saluaran Cerna Atas (I)Document58 pagesFmuntah Dan Obstruksi Saluaran Cerna Atas (I)irmaarmiyahNo ratings yet
- Aortic Disection KuliahDocument11 pagesAortic Disection KuliahdrnunungNo ratings yet
- Muntah Dan Obstruksi Saluaran Cerna Atas (I)Document48 pagesMuntah Dan Obstruksi Saluaran Cerna Atas (I)Amalia Hendar PangestutiNo ratings yet
- Causes and treatment of gastrointestinal bleeding in childrenDocument21 pagesCauses and treatment of gastrointestinal bleeding in childrenAmalia Hendar PangestutiNo ratings yet
- Humoral Immune Responses Dr. Ika YustisiaDocument45 pagesHumoral Immune Responses Dr. Ika YustisiaAmalia Hendar PangestutiNo ratings yet
- Hypertension and Heart FailureDocument74 pagesHypertension and Heart FailureMuhammad Syamil Rozlan100% (1)
- Chapter 6Document18 pagesChapter 6Amalia Hendar PangestutiNo ratings yet
- National Cardiovascular Center Harapan KitaDocument20 pagesNational Cardiovascular Center Harapan KitanurulrezqiaNo ratings yet
- Update in Nociceptive Pain TreatmentDocument48 pagesUpdate in Nociceptive Pain TreatmentAmalia Hendar PangestutiNo ratings yet
- Vitamin A - Adverse Effects - OverdoseDocument2 pagesVitamin A - Adverse Effects - OverdoseAmalia Hendar PangestutiNo ratings yet
- Small Group Learning (SGL) Bagian NeurologiDocument2 pagesSmall Group Learning (SGL) Bagian NeurologiAmalia Hendar PangestutiNo ratings yet
- Neurogenic BladderDocument36 pagesNeurogenic BladderAmalia Hendar PangestutiNo ratings yet
- JNC 8Document14 pagesJNC 8amiwahyuniNo ratings yet
- MahvanDocument7 pagesMahvanyasahswi91No ratings yet
- Small Group Learning (SGL) Bagian NeurologiDocument2 pagesSmall Group Learning (SGL) Bagian NeurologiAmalia Hendar PangestutiNo ratings yet
- 2018 World Traumatic Dental Injury Prevalence and IncidenceDocument16 pages2018 World Traumatic Dental Injury Prevalence and IncidencebaridinoNo ratings yet
- Extinction - WikipediaDocument14 pagesExtinction - Wikipediaskline3No ratings yet
- Chapter One - Understanding The Digital WorldDocument8 pagesChapter One - Understanding The Digital Worldlaith alakelNo ratings yet
- Japanese Tea Cups LessonDocument3 pagesJapanese Tea Cups Lessonapi-525048974No ratings yet
- GII-07 Training MaterialDocument191 pagesGII-07 Training MaterialIris Amati MartinsNo ratings yet
- Ns5e rw3 SB Ak HyeDocument24 pagesNs5e rw3 SB Ak HyeKeys Shield JoshuaNo ratings yet
- Umair Mazher ThesisDocument44 pagesUmair Mazher Thesisumair_mazherNo ratings yet
- VIII MKL Duet I Etap 2018 Angielski Arkusz Dla PiszącegoDocument5 pagesVIII MKL Duet I Etap 2018 Angielski Arkusz Dla PiszącegoKamilNo ratings yet
- Krashen's 5 Hypotheses of Second Language AcquisitionDocument69 pagesKrashen's 5 Hypotheses of Second Language Acquisitionabdo mohamedNo ratings yet
- Endocrine Hypothyroidism HyperthyroidismDocument16 pagesEndocrine Hypothyroidism HyperthyroidismJeel MohtaNo ratings yet
- People v Gemoya and Tionko - Supreme Court upholds murder convictionDocument7 pagesPeople v Gemoya and Tionko - Supreme Court upholds murder convictionLASNo ratings yet
- Mr. Honey's Large Business DictionaryEnglish-German by Honig, WinfriedDocument538 pagesMr. Honey's Large Business DictionaryEnglish-German by Honig, WinfriedGutenberg.orgNo ratings yet
- (Cambridge Series in Statistical and Probabilistic Mathematics) Gerhard Tutz, Ludwig-Maximilians-Universität Munchen - Regression For Categorical Data-Cambridge University Press (2012)Document574 pages(Cambridge Series in Statistical and Probabilistic Mathematics) Gerhard Tutz, Ludwig-Maximilians-Universität Munchen - Regression For Categorical Data-Cambridge University Press (2012)shu100% (2)
- Wjec Gcse English Literature Coursework Mark SchemeDocument6 pagesWjec Gcse English Literature Coursework Mark Schemef6a5mww8100% (2)
- Primer To Using Stampplot® Pro Standard User LicensedDocument21 pagesPrimer To Using Stampplot® Pro Standard User LicensedSandy Rachman AdrianNo ratings yet
- Homework WatergateDocument8 pagesHomework Watergateaapsujtif100% (1)
- Functional Appliances 2018Document45 pagesFunctional Appliances 2018tonhanrhmNo ratings yet
- Ch.24.2 Animal Evolution and DiversityDocument34 pagesCh.24.2 Animal Evolution and DiversityweldeenytNo ratings yet
- Answer Here:: FAMILY NAME - FIRST NAME - CLASSCODEDocument4 pagesAnswer Here:: FAMILY NAME - FIRST NAME - CLASSCODEUchayyaNo ratings yet
- Book Review Reclaim Your HeartDocument7 pagesBook Review Reclaim Your HeartShaheer KhanNo ratings yet
- Dreams and Destiny Adventure HookDocument5 pagesDreams and Destiny Adventure HookgravediggeresNo ratings yet
- School For Good and EvilDocument4 pagesSchool For Good and EvilHaizyn RizoNo ratings yet
- 7 Years - Lukas Graham SBJDocument2 pages7 Years - Lukas Graham SBJScowshNo ratings yet
- Louis Theroux PowerpointDocument6 pagesLouis Theroux Powerpointapi-330762792No ratings yet
- Culture of BMWDocument6 pagesCulture of BMWhk246100% (1)
- The Forty Nine StepsDocument312 pagesThe Forty Nine Stepsoldnic67% (3)
- Evelyn Nakano Glenn, "From Servitude To Service Work: Historical Continuities in The Racial Division of Paid Reproductive Labor"Document44 pagesEvelyn Nakano Glenn, "From Servitude To Service Work: Historical Continuities in The Racial Division of Paid Reproductive Labor"s0metim3sNo ratings yet
- ISE I Conversation Task - Rules and RegulationsDocument3 pagesISE I Conversation Task - Rules and RegulationsElena B. HerreroNo ratings yet
- Sustainability of A Beach Resort A Case Study-1Document6 pagesSustainability of A Beach Resort A Case Study-1abhinavsathishkumarNo ratings yet