You might also like
- Clinical Anatomy of Upper Limb Joints and MusclesDocument92 pagesClinical Anatomy of Upper Limb Joints and Musclesgechanatomy100% (1)
- Ultrasound of The ShoulderDocument15 pagesUltrasound of The ShoulderAndrei GianinaNo ratings yet
- Guyton & Hall Physiology Review 3rd Ed PDFDocument275 pagesGuyton & Hall Physiology Review 3rd Ed PDFDhiya Muthiah Gaffari94% (36)
- Risk Ass - CE - 0994 - GAS CUTTING, WELDING, GRINDING, LOADING AND UNLOADING OF ANODE PALETTEDocument12 pagesRisk Ass - CE - 0994 - GAS CUTTING, WELDING, GRINDING, LOADING AND UNLOADING OF ANODE PALETTEnsadnan100% (4)
- Assessment MusculoskeletalDocument6 pagesAssessment Musculoskeletaldd marshall100% (1)
- Rotator Cuff InjuryDocument29 pagesRotator Cuff InjuryArko duttaNo ratings yet
- THE ELDER SCROLLS - Oblivion - GuideDocument330 pagesTHE ELDER SCROLLS - Oblivion - GuideMelanieReyesNo ratings yet
- Shoulder Assessment: Ayesha RazzaqDocument47 pagesShoulder Assessment: Ayesha RazzaqayeshaNo ratings yet
- Balance Skeletal Traction1Document31 pagesBalance Skeletal Traction1Maria Victoria ColomaNo ratings yet
- Pyshical Examination OrthopaediDocument67 pagesPyshical Examination OrthopaediSheryl ElitaNo ratings yet
- Rotator Cuff TendynopatyDocument10 pagesRotator Cuff TendynopatyDipo SiahaanNo ratings yet
- D9 P.B PDFDocument885 pagesD9 P.B PDFDe Javu100% (1)
- William C. Cottrell, MD AbstractDocument4 pagesWilliam C. Cottrell, MD AbstractmalaNo ratings yet
- GALS AssessmentDocument46 pagesGALS AssessmentdrindrasNo ratings yet
- Israel Football PhilosophyDocument36 pagesIsrael Football PhilosophyAzamat AsanbekovNo ratings yet
- SotDL - Spell Cards - SotDL PathDocument18 pagesSotDL - Spell Cards - SotDL PathIzael Evangelista100% (1)
- Musculoskeletal Exam Teaching OutlineDocument12 pagesMusculoskeletal Exam Teaching OutlineAngeliki KostakiNo ratings yet
- ElbowDocument7 pagesElbowapi-302398226No ratings yet
- The Painful Shoulder - Part I. Clinical Evaluation PDFDocument17 pagesThe Painful Shoulder - Part I. Clinical Evaluation PDFOscar FrizziNo ratings yet
- Alekhine With 4.a4 PDFDocument16 pagesAlekhine With 4.a4 PDFrubenkeller5204No ratings yet
- Supraspinatus TendinitisDocument7 pagesSupraspinatus Tendinitismilananand100% (1)
- LymphaticDocument52 pagesLymphaticlemuel_queNo ratings yet
- Lesões de Punho e MãoDocument86 pagesLesões de Punho e MãoRobsom InacioNo ratings yet
- KnittingLabShop DollAgneshkaDocument27 pagesKnittingLabShop DollAgneshkacharlotte91% (22)
- Efficacy of Sot in FemalesDocument7 pagesEfficacy of Sot in FemalesDenise MathreNo ratings yet
- Shoulder Pain - The Supraspinatous MuscleDocument6 pagesShoulder Pain - The Supraspinatous Musclesale18100% (1)
- Shoulder ExamDocument24 pagesShoulder ExamMuhammad FahmyNo ratings yet
- Presentation1 150221070554 Conversion Gate01Document75 pagesPresentation1 150221070554 Conversion Gate01yellymarlianapatuNo ratings yet
- Case Report Presentation - TFCCDocument3 pagesCase Report Presentation - TFCCapi-414663729No ratings yet
- Fraktur HumerusDocument7 pagesFraktur HumerusAnggoro DwiNo ratings yet
- Musculoskeletal HandoutDocument9 pagesMusculoskeletal HandoutwanttobemdplzNo ratings yet
- Assessment SpineDocument8 pagesAssessment Spineزيد مسعودNo ratings yet
- The Forearm, Wrist and HandDocument20 pagesThe Forearm, Wrist and HandKatalinNo ratings yet
- 6 Elbow and WristDocument76 pages6 Elbow and Wristalinaziyad3No ratings yet
- Physical Examination of Musculoskeletal System 2021Document50 pagesPhysical Examination of Musculoskeletal System 2021RPMFA RPMFANo ratings yet
- Aco102 085dDocument2 pagesAco102 085dDonny HendrawanNo ratings yet
- (OSCE) (Checklist) Hip ExaminationDocument7 pages(OSCE) (Checklist) Hip ExaminationastarimediantoNo ratings yet
- The Knee Is One of The More Commonly Injured JointsDocument4 pagesThe Knee Is One of The More Commonly Injured JointslieNo ratings yet
- Scapular Ax in NeuroDocument6 pagesScapular Ax in NeurolavanyaphdNo ratings yet
- Essay 6Document26 pagesEssay 6Cheong Yee WengNo ratings yet
- Checklist Hip ExaminationDocument7 pagesChecklist Hip ExaminationJavednNo ratings yet
- Checklist Hip ExaminationDocument8 pagesChecklist Hip Examinationhakuna matataNo ratings yet
- NutriDocument6 pagesNutri002No ratings yet
- Checklist Pemeriksaan Fisik Pada HIP (OSCE) : PendahuluanDocument3 pagesChecklist Pemeriksaan Fisik Pada HIP (OSCE) : PendahuluanFelix joviandiNo ratings yet
- Clavicle FractureDocument27 pagesClavicle FractureOves Patni100% (1)
- Club Hand RibkaDocument31 pagesClub Hand RibkaRibka TheodoraNo ratings yet
- Shoulder Pain IDocument5 pagesShoulder Pain Iunbelievable686No ratings yet
- Acromioplasty Rehab ProtocolDocument3 pagesAcromioplasty Rehab ProtocolJay RammaNo ratings yet
- Arthroscopy of The Wrist - Anatomy and TechniqueDocument4 pagesArthroscopy of The Wrist - Anatomy and TechniqueDiego Maté MartínNo ratings yet
- Part A: Introduction To The Surface Anatomy of The Thoracic SpineDocument11 pagesPart A: Introduction To The Surface Anatomy of The Thoracic SpineHammad -ullahNo ratings yet
- Orthopedic Assessment Sample PDFDocument11 pagesOrthopedic Assessment Sample PDFSyahrani SaidNo ratings yet
- Ultt26 03 2020 231022061259 7f0a393fDocument24 pagesUltt26 03 2020 231022061259 7f0a393fSri Ram 07No ratings yet
- MFR Functional TestingDocument0 pagesMFR Functional TestingasloocltNo ratings yet
- Dr. Ashish Research ProposalDocument14 pagesDr. Ashish Research ProposalShobhit RaoNo ratings yet
- Musculoskeletal Ultrasound Technical GuidelinesDocument43 pagesMusculoskeletal Ultrasound Technical GuidelinesMarco VincentiNo ratings yet
- Epidemiology of Shoulder PainDocument58 pagesEpidemiology of Shoulder PainniekoNo ratings yet
- President's Address: Trick MovementsDocument3 pagesPresident's Address: Trick MovementsDr. Rushikesh K. Joshi100% (1)
- Shoulder DislocationDocument12 pagesShoulder DislocationSam Witwicky50% (2)
- Flexibility TestingDocument13 pagesFlexibility Testingمحمد عقلNo ratings yet
- Textbook Impingement SyndromeDocument28 pagesTextbook Impingement SyndromeQueenBalqisNo ratings yet
- Supraspinatus Tendon Tears: Comparison of US and MR Arthrography With Surgical CorrelationDocument7 pagesSupraspinatus Tendon Tears: Comparison of US and MR Arthrography With Surgical CorrelationStephen WestNo ratings yet
- Upload Scribd 4Document7 pagesUpload Scribd 4Yoga AninditaNo ratings yet
- Stiff Elbow PP Nov 14Document35 pagesStiff Elbow PP Nov 14BekNo ratings yet
- Shoulder Dislocation Background: Shoulder Dislocations Traumatic InjuryDocument7 pagesShoulder Dislocation Background: Shoulder Dislocations Traumatic Injuryanastasiaanggita_265No ratings yet
- Clinical Tests in Shoulder Examination - How To Perform ThemDocument7 pagesClinical Tests in Shoulder Examination - How To Perform Themprofpt98No ratings yet
- A Manual of the Operations of Surgery: For the Use of Senior Students, House Surgeons, and Junior PractitionersFrom EverandA Manual of the Operations of Surgery: For the Use of Senior Students, House Surgeons, and Junior PractitionersNo ratings yet
- Fcps SurgeryDocument1 pageFcps SurgeryMohsin SarwarNo ratings yet
- Eom McqsDocument2 pagesEom McqsMohsin SarwarNo ratings yet
- First Aid Cardiovascular TestDocument17 pagesFirst Aid Cardiovascular TestZeeshan AbdulNasirNo ratings yet
- Fcps SurgeryDocument1 pageFcps SurgeryMohsin SarwarNo ratings yet
- FcpsDocument1 pageFcpsMohsin SarwarNo ratings yet
- Games at MazedaDocument7 pagesGames at MazedaMuhib H AdilNo ratings yet
- Hometown - Kaslo & AreaDocument8 pagesHometown - Kaslo & AreaPennywise PublishingNo ratings yet
- XBX IDocument5 pagesXBX IdanieloscmNo ratings yet
- Air - Shawn Mendes (Chords)Document3 pagesAir - Shawn Mendes (Chords)Courtney DizonNo ratings yet
- LB State Roste and Schedule 2010Document2 pagesLB State Roste and Schedule 2010Rich WilliamsNo ratings yet
- Avenger 1 Play ImporDocument12 pagesAvenger 1 Play ImporJosé ChamayNo ratings yet
- Suspension and AxleDocument100 pagesSuspension and AxleChristian Linares AbreuNo ratings yet
- Gate Aerospace 2018 SolutionDocument35 pagesGate Aerospace 2018 SolutionJackobNo ratings yet
- AbbaDocument3 pagesAbbaMina CesarNo ratings yet
- 610 Game Plan TemplateDocument71 pages610 Game Plan TemplateBillAustinNo ratings yet
- UnitedPerfumes Catalog With Prices SPNDocument100 pagesUnitedPerfumes Catalog With Prices SPNSandra RiañoNo ratings yet
- 1.5.2 Hookes Law Set 1 MsDocument7 pages1.5.2 Hookes Law Set 1 MsKoser IrshadNo ratings yet
- The History of AthleticsDocument59 pagesThe History of AthleticsLev Mazed SulioNo ratings yet
- SpellbookDocument1 pageSpellbookEmilie DelageNo ratings yet
- Asruddin's AimDocument9 pagesAsruddin's AimNewstar ComputersNo ratings yet
- Shakira Isabel Mebarak RipollDocument18 pagesShakira Isabel Mebarak RipollAngela SanchezNo ratings yet
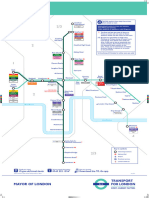
- DLR Route MapDocument1 pageDLR Route MapChristopher HollowayNo ratings yet
- 4he75m Part ListDocument6 pages4he75m Part ListJvlValenzuelaNo ratings yet
- English 1119 Trial PaperDocument23 pagesEnglish 1119 Trial Paperyogamalar_chandrasekaranNo ratings yet
- UEFA Champions League Anthem Piano TutorialDocument4 pagesUEFA Champions League Anthem Piano TutorialSanmarkioMarkioNo ratings yet
- Coxarthrosis: Patient InformationDocument1 pageCoxarthrosis: Patient InformationBlanchette ChNo ratings yet
- Examen Final - Semana 8 - ESP - SEGUNDO BLOQUE-INGLES GENERAL II - (GRUPO2)Document16 pagesExamen Final - Semana 8 - ESP - SEGUNDO BLOQUE-INGLES GENERAL II - (GRUPO2)Alex AlegriaNo ratings yet
- Hotel Details: Inr 6,500 Per PersonDocument3 pagesHotel Details: Inr 6,500 Per PersonMayank BhattNo ratings yet