You might also like
- The Placenta BDocument48 pagesThe Placenta BLulano MbasuNo ratings yet
- Placenta and Amniotic Fluid Structure FunctionDocument52 pagesPlacenta and Amniotic Fluid Structure FunctionDoli P Hutauruk100% (1)
- Assessment of PlacentaDocument21 pagesAssessment of PlacentaAarti RajputNo ratings yet
- Embryology, Pathophysiology, and Ultrasound Characteristics of The Placenta ObjectivesDocument13 pagesEmbryology, Pathophysiology, and Ultrasound Characteristics of The Placenta ObjectivesAudrey100% (5)
- Placenta and Placental Hormones Lecture+PPT PDFDocument29 pagesPlacenta and Placental Hormones Lecture+PPT PDFPamela Marie Cope100% (1)
- Implantation and PlacentaDocument52 pagesImplantation and PlacentaMs BadooNo ratings yet
- Placenta FunctionsDocument46 pagesPlacenta Functionsvenkata sryanamala50% (2)
- PLACENTA STRUCTURE AND FUNCTIONDocument33 pagesPLACENTA STRUCTURE AND FUNCTIONAya KamajayaNo ratings yet
- The Antenatal Care-maternal Changes During Pregnancy 7Document75 pagesThe Antenatal Care-maternal Changes During Pregnancy 795kscbyqxmNo ratings yet
- PlacentaDocument11 pagesPlacentasubashikNo ratings yet
- Perkembangan Plasenta (Autosaved) .En - IdDocument18 pagesPerkembangan Plasenta (Autosaved) .En - IdFATIMAHNo ratings yet
- ch.8 Embryo PDFDocument22 pagesch.8 Embryo PDFMohammad GhannamNo ratings yet
- Maternal Placental Foetal UnitDocument10 pagesMaternal Placental Foetal UnitFestus SinoNo ratings yet
- Case Study of Cesarean SectionDocument9 pagesCase Study of Cesarean SectionErika Joy Imperio0% (1)
- Fetal and Placental Development - FETAL Sac, Umbilical Cord .Abnormalities of PlacentaDocument150 pagesFetal and Placental Development - FETAL Sac, Umbilical Cord .Abnormalities of PlacentaKripa SusanNo ratings yet
- The Growing FetusDocument62 pagesThe Growing Fetuscoosa liquorsNo ratings yet
- Fertilization and ImplantationDocument3 pagesFertilization and ImplantationTandingco, Olivia Mari H.No ratings yet
- Unit 2 - Fertilization, Impantation, Development of Placenta and Its Function, AbnormalityDocument62 pagesUnit 2 - Fertilization, Impantation, Development of Placenta and Its Function, AbnormalityN. Siva100% (1)
- Breast Diseases: Detection and Physical ExamDocument22 pagesBreast Diseases: Detection and Physical ExamnicewanNo ratings yet
- Lecture 1physiology of PregnancyDocument58 pagesLecture 1physiology of PregnancyОлександра ЗагородняNo ratings yet
- Placental Development - Implantation - Transfer - Clinical RelevanceDocument3 pagesPlacental Development - Implantation - Transfer - Clinical RelevanceLiridon SopajNo ratings yet
- Fetal Membranes and PlacentaDocument53 pagesFetal Membranes and PlacentaALFAHRUL CAHYADINo ratings yet
- 10 Placenta DR - GosaiDocument29 pages10 Placenta DR - GosaiDr.B.B.GosaiNo ratings yet
- Pathology of Preeclampsia (Autosaved) (Autosaved)Document59 pagesPathology of Preeclampsia (Autosaved) (Autosaved)ck4realNo ratings yet
- Placenta & Fetal CirculationDocument32 pagesPlacenta & Fetal CirculationFarxan Da Napolian BwoyNo ratings yet
- Embryological and fetal development seminarDocument30 pagesEmbryological and fetal development seminarMSc. PreviousNo ratings yet
- Case Study - CS With BTLDocument16 pagesCase Study - CS With BTLAJ Roze Holmes100% (2)
- Chapter 9: Nursing Care During Normal Pregnancy and Care of The Developing FetusDocument8 pagesChapter 9: Nursing Care During Normal Pregnancy and Care of The Developing FetusAlyssaGrandeMontimor100% (1)
- THE Process OF Conceptio NDocument21 pagesTHE Process OF Conceptio NGregory LitangNo ratings yet
- Congenital Abnormalities of The UterusDocument7 pagesCongenital Abnormalities of The Uterusمحمود الموسويNo ratings yet
- Pregnancy Health Promotion and DevelopmentDocument11 pagesPregnancy Health Promotion and DevelopmentKathy Wollschleger100% (1)
- Maternal and Child Health IDocument772 pagesMaternal and Child Health Ikarendelarosa06100% (6)
- Functional Anatomy - Part II: Uterus, Fetal Circulation & Male Reproductive Organ Selected VariationsDocument69 pagesFunctional Anatomy - Part II: Uterus, Fetal Circulation & Male Reproductive Organ Selected Variationshfkxbbbty2No ratings yet
- The PlacentaDocument3 pagesThe PlacentaLiezelNo ratings yet
- Stages of Fetal Growth and DevelopmentDocument10 pagesStages of Fetal Growth and DevelopmentGrant KhangabNo ratings yet
- Parturition, Foetal Membranes and Multiple PregnanciesDocument38 pagesParturition, Foetal Membranes and Multiple PregnanciesGeoffreyNo ratings yet
- Fertilization: Glora P. de Leon, RN, RM, ManDocument103 pagesFertilization: Glora P. de Leon, RN, RM, ManJoan VillafrancaNo ratings yet
- Fetal CirculationDocument28 pagesFetal CirculationNelai GoNo ratings yet
- Lect12 - Amniotic Fluid ModifiedDocument22 pagesLect12 - Amniotic Fluid Modifiedyelisetti DakshayaniNo ratings yet
- Charles Z. Ariola JR., MSN., LPT, Rn. Instructor IDocument22 pagesCharles Z. Ariola JR., MSN., LPT, Rn. Instructor ICharlz ZipaganNo ratings yet
- Normal PregnancyDocument86 pagesNormal PregnancygayleesinfuegoNo ratings yet
- Fetal DevelopmentDocument26 pagesFetal DevelopmentyuddNo ratings yet
- Maternal and Child Health Nursing (NCM 101 Lect) Part 1Document4 pagesMaternal and Child Health Nursing (NCM 101 Lect) Part 1yunjung0518100% (7)
- 2.development of Normal PlacentaDocument55 pages2.development of Normal PlacentapriyaNo ratings yet
- FertilizationDocument6 pagesFertilizationKristine Castillo100% (1)
- Umblical Cord AbnormalitiesDocument54 pagesUmblical Cord AbnormalitiesKeerti Patel100% (5)
- MCN Nursing 1Document107 pagesMCN Nursing 1Fau Fau DheoboNo ratings yet
- 1.1c Implantation & Placental DevelopmentDocument5 pages1.1c Implantation & Placental DevelopmentBea Samonte100% (1)
- 10 - PlacentaDocument21 pages10 - Placentaalejosshht100% (1)
- 11th Lecture Amnion& Amniotic FluidDocument35 pages11th Lecture Amnion& Amniotic FluidHussein Al Saedi100% (1)
- Fetal Membranes ExplainedDocument26 pagesFetal Membranes ExplainedSubham YadavNo ratings yet
- Care of The Mother and The FetusDocument99 pagesCare of The Mother and The FetusBea Bianca CruzNo ratings yet
- OR Write-Up CSDocument13 pagesOR Write-Up CSalex_tan1981No ratings yet
- Endocrine Function of PlacentaDocument4 pagesEndocrine Function of PlacentaArabelle GONo ratings yet
- 1-4 Fertilization & Fetal DevelopmentDocument9 pages1-4 Fertilization & Fetal DevelopmentElla DionedaNo ratings yet
- Pathologies of The Amniotic Fluid Volume: Prepared by DR N. Med. Radosław Blok - I Katedra Gin - Poł. AM WrocławDocument56 pagesPathologies of The Amniotic Fluid Volume: Prepared by DR N. Med. Radosław Blok - I Katedra Gin - Poł. AM WrocławSupreet Singh MalhiNo ratings yet
- 1-Prenatal & Fetal Development-93666Document45 pages1-Prenatal & Fetal Development-93666Izziddin YassineNo ratings yet
- Place Ntation 2Document38 pagesPlace Ntation 2Dr. Vinay VijayakumarNo ratings yet
- PLA-FET CIRDocument38 pagesPLA-FET CIRDr. Vinay VijayakumarNo ratings yet
- Last Minute Embryology: Human embryology made easy and digestible for medical and nursing studentsFrom EverandLast Minute Embryology: Human embryology made easy and digestible for medical and nursing studentsNo ratings yet
- Maternity Nursing Lecture NotesDocument198 pagesMaternity Nursing Lecture Notesprogramgrabber75% (4)
- The Growing FetusDocument62 pagesThe Growing Fetuscoosa liquorsNo ratings yet
- Menorrhagia (Heavy Menstrual Bleeding)Document55 pagesMenorrhagia (Heavy Menstrual Bleeding)Aizi DwimeilaNo ratings yet
- The POCSO Act & Adolescents' Access To Abortion in India Heightened Vulnerabilities, Health Risks, and Impact On Their RightsDocument8 pagesThe POCSO Act & Adolescents' Access To Abortion in India Heightened Vulnerabilities, Health Risks, and Impact On Their RightsClara SelviNo ratings yet
- Patient Brochure - Mirena® IUDDocument24 pagesPatient Brochure - Mirena® IUDjair basantesNo ratings yet
- Presented By-Ms. Nidhi Shukla M.Sc. Nursing 1 YearDocument43 pagesPresented By-Ms. Nidhi Shukla M.Sc. Nursing 1 YearFajar Islam SitanggangNo ratings yet
- If Men Could MenstruateDocument3 pagesIf Men Could Menstruatepigixih621No ratings yet
- TOG Evolution in Screening For Down SyndromeDocument7 pagesTOG Evolution in Screening For Down SyndromeMarNo ratings yet
- MODULE 4 1st Part INTRAPARTAL CARE - Docx 2Document13 pagesMODULE 4 1st Part INTRAPARTAL CARE - Docx 2jared abriolNo ratings yet
- Jurnal - Ferdi Adi Pratama - 195050100111049Document10 pagesJurnal - Ferdi Adi Pratama - 195050100111049tps9girimulyoNo ratings yet
- Part, Function and Process of Reproduction SystemDocument31 pagesPart, Function and Process of Reproduction SystemSavia NaldiNo ratings yet
- CPD: Cephalo-Pelvic Disproportion PathophysiologyDocument3 pagesCPD: Cephalo-Pelvic Disproportion PathophysiologyTeanne Bathan100% (1)
- Penile Length-Somatometric Parameters Relationship in Healthy Egyptian MenDocument5 pagesPenile Length-Somatometric Parameters Relationship in Healthy Egyptian Mengohary18047No ratings yet
- Gyne Lecture NoteDocument572 pagesGyne Lecture NoteMRT RadiologyNo ratings yet
- Healthcare Industry Quiz-1: For Answers Click HereDocument2 pagesHealthcare Industry Quiz-1: For Answers Click HereSantosh JSENo ratings yet
- The Process of ReproductionDocument5 pagesThe Process of ReproductionNamie DagNo ratings yet
- Treating Recurrent Miscarriage with Traditional Chinese MedicineDocument12 pagesTreating Recurrent Miscarriage with Traditional Chinese MedicineLecery Sophia WongNo ratings yet
- Ncm107j Weekly NotesDocument11 pagesNcm107j Weekly NotesSHEENA MAE DE LOS REYESNo ratings yet
- Hubungan Aktivitas Olahraga dengan Sindrom Pramenstruasi pada RemajaDocument120 pagesHubungan Aktivitas Olahraga dengan Sindrom Pramenstruasi pada RemajaauliaNo ratings yet
- Human Sphere and Population GrowthDocument21 pagesHuman Sphere and Population Growthfredpaul espero100% (2)
- Topic 6 - Imperfect Cause DefectDocument2 pagesTopic 6 - Imperfect Cause DefectSyaza Izzah Athirah Bt SpaieeNo ratings yet
- Embryology - The First WeekDocument51 pagesEmbryology - The First WeekLugembe MasolaNo ratings yet
- AOGD Bulletin November 2019Document64 pagesAOGD Bulletin November 2019Kavitha NarayanaswamyNo ratings yet
- Incidence of Candidiasis Amongst Female Students of A Tertiary Institution in Rivers State NigeriaDocument6 pagesIncidence of Candidiasis Amongst Female Students of A Tertiary Institution in Rivers State NigeriaUbali Ibrahim HashimuNo ratings yet
- Institute of Nursing and Allied Health SciencesDocument2 pagesInstitute of Nursing and Allied Health SciencesCristin UngabNo ratings yet
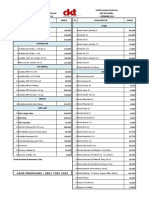
- DKT Indonesia Daftar Harga Produk Kontrasepsi 1 September 2018Document4 pagesDKT Indonesia Daftar Harga Produk Kontrasepsi 1 September 2018YuliantiNo ratings yet
- Definition ContraceptionDocument4 pagesDefinition Contraceptionmarlon marlon JuniorNo ratings yet
- Occipito Posterior (PositionDocument44 pagesOccipito Posterior (PositionArambam Aruna100% (6)
- Condom - Google SearchDocument1 pageCondom - Google Searchlive hacksNo ratings yet
- Thesis Abortion Research PaperDocument6 pagesThesis Abortion Research Paperstefanieyangmanchester100% (2)