You might also like
- THR Definitions, Anatomy, Causes, Description & ExercisesDocument22 pagesTHR Definitions, Anatomy, Causes, Description & ExercisesAnonymous dGfXuDd5No ratings yet
- CTEVDocument61 pagesCTEVSylvia LoongNo ratings yet
- Hemiarthroplasty Hip - Apr20Document10 pagesHemiarthroplasty Hip - Apr20Shalu OjhaNo ratings yet
- Pes Cavus: Eka Anggraini Padma Vidya GayatriDocument13 pagesPes Cavus: Eka Anggraini Padma Vidya GayatriPadma VidyaNo ratings yet
- Hand and Wrist PathwayDocument2 pagesHand and Wrist PathwaydrsadafrafiNo ratings yet
- Tuberculosis of Hip JointDocument25 pagesTuberculosis of Hip JointYousra ShaikhNo ratings yet
- Biomechanics Ankle PresentationDocument10 pagesBiomechanics Ankle Presentationx.cortez100% (1)
- Patellar FractureDocument25 pagesPatellar FractureSyafiq ShahbudinNo ratings yet
- Aaop2003 PDFDocument102 pagesAaop2003 PDFSalemNo ratings yet
- Club Foot-Dr J SahooDocument9 pagesClub Foot-Dr J SahooSheel Gupta100% (1)
- Prosthetic Case PresentationsDocument19 pagesProsthetic Case PresentationsptannenbaumNo ratings yet
- Clinical Examination of Hip JointDocument71 pagesClinical Examination of Hip JointDeevi Mohana SasankNo ratings yet
- Biomech of Hip JointDocument68 pagesBiomech of Hip JointkashifNo ratings yet
- BFO-Ankle Foot Orthotics - Introduction and Biomechanical PrinciplesDocument9 pagesBFO-Ankle Foot Orthotics - Introduction and Biomechanical PrinciplesnovitaNo ratings yet
- Biomechanics of GaitDocument27 pagesBiomechanics of Gaitsebastiao_est3197No ratings yet
- Ankel Heel PainDocument51 pagesAnkel Heel PainMeno Ali100% (1)
- Continuous Passive Motion Device BenefitsDocument9 pagesContinuous Passive Motion Device BenefitsAjay DherwaniNo ratings yet
- Principles of Tendon Transfer in The Hand and ForearmDocument9 pagesPrinciples of Tendon Transfer in The Hand and Forearm'Ema Surya PertiwiNo ratings yet
- Tennis ElbowDocument13 pagesTennis ElbowPadma PadalNo ratings yet
- Rehabilitation: Walking After Total Knee ReplacementDocument10 pagesRehabilitation: Walking After Total Knee ReplacementSandeep DhimanNo ratings yet
- Basic Principles of Tendon TransferDocument10 pagesBasic Principles of Tendon TransferyeapdshengNo ratings yet
- Erbs PalsyDocument9 pagesErbs PalsyVatsalVermaNo ratings yet
- CTEVDocument27 pagesCTEVJevisco LauNo ratings yet
- Amputation: Sites of Amputation: UEDocument6 pagesAmputation: Sites of Amputation: UEChristine PilarNo ratings yet
- Pinky - Plantar FasciitisDocument34 pagesPinky - Plantar FasciitisRavindra choudharyNo ratings yet
- Introduction PhysiotherapistDocument12 pagesIntroduction Physiotherapistapi-371068989No ratings yet
- Fracture ManagementDocument186 pagesFracture ManagementAyi SuwarayiNo ratings yet
- Examination of The Hip Joint - RP's Ortho NotesDocument5 pagesExamination of The Hip Joint - RP's Ortho NotesSabari NathNo ratings yet
- Lower Back Pain Causes and TreatmentsDocument19 pagesLower Back Pain Causes and TreatmentsGavin TessierNo ratings yet
- CTEVDocument17 pagesCTEVamal.fathullah100% (1)
- Prosthetic Knee Joints: Submitted By:-Ravi Mpo 1 YrDocument37 pagesProsthetic Knee Joints: Submitted By:-Ravi Mpo 1 YrRavi KumarNo ratings yet
- AmputationsDocument141 pagesAmputationsdeepaseira2205100% (2)
- Biomechanics & Pathomechanics of HandDocument81 pagesBiomechanics & Pathomechanics of HandAmrita L. Tomar67% (3)
- Rehabilitation protocol for mallet finger and zone injuriesDocument18 pagesRehabilitation protocol for mallet finger and zone injuriesaparnaNo ratings yet
- Mobility Aids With VideoDocument92 pagesMobility Aids With VideoRadha KrishnanNo ratings yet
- Cast and TractionDocument7 pagesCast and Tractionnamme01_margateNo ratings yet
- Soft tissue injury treatment RICEDocument2 pagesSoft tissue injury treatment RICEDenis Edem Dzebre100% (1)
- Shweta Aggarwal - Physiotherapy in Musculoskeletal ConditionsDocument283 pagesShweta Aggarwal - Physiotherapy in Musculoskeletal Conditionssaurav.das2030100% (1)
- CKC vs OKC Exercises - Functional Strength TrainingDocument2 pagesCKC vs OKC Exercises - Functional Strength Traininginrmpt77No ratings yet
- Thesis TopicDocument5 pagesThesis TopicSrikant KonchadaNo ratings yet
- Perthes Disease: A Rare Childhood Hip ConditionDocument4 pagesPerthes Disease: A Rare Childhood Hip ConditionMohamed HamoodNo ratings yet
- Manual Muscle Testing: Grade Value DescriptionDocument40 pagesManual Muscle Testing: Grade Value Descriptionjoanna gurtizaNo ratings yet
- Lower Limb Orthosis: Dr. Sumit Raghav, PT Assistant Professor Jyotirao Subharti College of PhysiotherapyDocument56 pagesLower Limb Orthosis: Dr. Sumit Raghav, PT Assistant Professor Jyotirao Subharti College of PhysiotherapyKavya Mittal100% (2)
- Orthotic Prescription Factors for KAFODocument54 pagesOrthotic Prescription Factors for KAFOFERYANDA UTAMI100% (1)
- TKR ProtocolDocument8 pagesTKR ProtocolSandeep SoniNo ratings yet
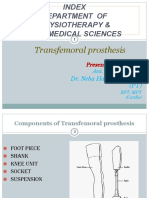
- TRANSFEMORAL - PPT 1Document64 pagesTRANSFEMORAL - PPT 1Farheen KhanNo ratings yet
- Endo'S: Surgical TechniqueDocument8 pagesEndo'S: Surgical Techniquefelipefernandezm5105No ratings yet
- Biomechanics of Knee Complex 1Document34 pagesBiomechanics of Knee Complex 1Dibyendunarayan BidNo ratings yet
- Lecture 1 Knee OrthosesDocument50 pagesLecture 1 Knee OrthosesAlfred JacksonNo ratings yet
- Rehabilitation of Adults With Upper-Limb AmputationsDocument59 pagesRehabilitation of Adults With Upper-Limb AmputationsSameeha AbbassNo ratings yet
- Physiotherapy Exercises After Abdominal SurgeryDocument32 pagesPhysiotherapy Exercises After Abdominal SurgeryHUZAIFA YAMAANNo ratings yet
- Elbow Joint CHP 10 PDFDocument42 pagesElbow Joint CHP 10 PDFAlfionita WikaNo ratings yet
- Hip Examination in The ChildDocument24 pagesHip Examination in The ChildDharmendra WidetyaNo ratings yet
- BankartDocument14 pagesBankartshayneberry25No ratings yet
- Floor Reaction Orthosis for Quadriceps WeaknessDocument45 pagesFloor Reaction Orthosis for Quadriceps WeaknessJipin Gopi100% (1)
- PCL Reconstruction Rehab ProtocolDocument19 pagesPCL Reconstruction Rehab ProtocolosamadrNo ratings yet
- Distal Biceps Repair Rehabilitation Protocol by Tendayi MutsopotsiDocument5 pagesDistal Biceps Repair Rehabilitation Protocol by Tendayi MutsopotsiPhysiotherapy Care SpecialistsNo ratings yet
- The Spencer TechniqueDocument11 pagesThe Spencer TechniqueDavidAgelliNo ratings yet
- DeQuervain Disease, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandDeQuervain Disease, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- The Effectiveness of Extracorporeal Shockwave Therapy in Common Lower Limb Conditions (PDFDrive)Document22 pagesThe Effectiveness of Extracorporeal Shockwave Therapy in Common Lower Limb Conditions (PDFDrive)akheel ahammedNo ratings yet
- Spinal Exercises: Information For PatientsDocument12 pagesSpinal Exercises: Information For Patientsakheel ahammedNo ratings yet
- Dry Needling For Manual Therapists Points, Techniques and TreatmentsDocument316 pagesDry Needling For Manual Therapists Points, Techniques and Treatmentszokim100% (6)
- Joint Pain Leaflet PDFDocument12 pagesJoint Pain Leaflet PDFSuaeni Kurnia Wirda100% (1)
- SWDDocument58 pagesSWDakheel ahammedNo ratings yet
- Partial and Total Knee Arthroplasty Home Exercise ProgramDocument7 pagesPartial and Total Knee Arthroplasty Home Exercise Programakheel ahammedNo ratings yet
- Upper Body Thera Band Exercise Program - BasicDocument7 pagesUpper Body Thera Band Exercise Program - Basicakheel ahammed100% (1)
- Physiotherapy Management of TMJ PainDocument4 pagesPhysiotherapy Management of TMJ Painakheel ahammed100% (1)
- NEW! - Mushahwar - Restoring Locomotion by Arm Cycling and Electrical Stimulation After SCI HandoutDocument13 pagesNEW! - Mushahwar - Restoring Locomotion by Arm Cycling and Electrical Stimulation After SCI Handoutakheel ahammedNo ratings yet
- NEW! - Mushahwar - Restoring Locomotion by Arm Cycling and Electrical Stimulation After SCI HandoutDocument13 pagesNEW! - Mushahwar - Restoring Locomotion by Arm Cycling and Electrical Stimulation After SCI Handoutakheel ahammedNo ratings yet
- DNS PDFDocument12 pagesDNS PDFMaksim BogdanovNo ratings yet
- User Manual: Therapy SystemsDocument13 pagesUser Manual: Therapy Systemsakheel ahammedNo ratings yet
- Physiotherapy in Gastrectomy CholecystectomyDocument19 pagesPhysiotherapy in Gastrectomy Cholecystectomyakheel ahammedNo ratings yet
- Bessfrozen2016 160429143358Document45 pagesBessfrozen2016 160429143358akheel ahammedNo ratings yet
- H Vac Electrode EnglishDocument20 pagesH Vac Electrode Englishakheel ahammedNo ratings yet
- Nursing Care of Genitourinary Disorders: Kidney and Nephron FunctionDocument72 pagesNursing Care of Genitourinary Disorders: Kidney and Nephron Functionakheel ahammedNo ratings yet
- Shock Wave Clinical NotesDocument122 pagesShock Wave Clinical Notesakheel ahammedNo ratings yet
- Introduction To Physiotherapy in General Surgical ConditionsDocument20 pagesIntroduction To Physiotherapy in General Surgical Conditionsakheel ahammedNo ratings yet
- Guaranteed How To Get WomenDocument56 pagesGuaranteed How To Get Womenakheel ahammedNo ratings yet
- Liver Transplantation OverviewDocument100 pagesLiver Transplantation Overviewakheel ahammedNo ratings yet
- Introduction To Physiotherapy in General Surgical ConditionsDocument20 pagesIntroduction To Physiotherapy in General Surgical Conditionsakheel ahammedNo ratings yet
- Understanding Anaesthesia For PhysiotherapistDocument28 pagesUnderstanding Anaesthesia For Physiotherapistakheel ahammedNo ratings yet
- Common Operations PhysiotherapyDocument83 pagesCommon Operations Physiotherapyakheel ahammedNo ratings yet
- Developments in Neurological RehabilitationDocument39 pagesDevelopments in Neurological Rehabilitationakheel ahammedNo ratings yet
- Physiotherapy Guide for Pain Relief and RehabilitationDocument42 pagesPhysiotherapy Guide for Pain Relief and Rehabilitationakheel ahammedNo ratings yet
- Child Abuse and Neglect:: Recognizing, Reporting, and Responding in Early ChildhoodDocument45 pagesChild Abuse and Neglect:: Recognizing, Reporting, and Responding in Early Childhoodakheel ahammedNo ratings yet
- Presentation On Advertisement Campaign......Document24 pagesPresentation On Advertisement Campaign......Kavita SharmaNo ratings yet
- Diabetes AwarenessDocument27 pagesDiabetes Awarenessakheel ahammedNo ratings yet
- Understanding and Living With Chronic PainDocument68 pagesUnderstanding and Living With Chronic Painakheel ahammedNo ratings yet
- Diabetes Training For School Employees 3Document48 pagesDiabetes Training For School Employees 3akheel ahammedNo ratings yet
- Bronchiectasis Guide: Causes, Symptoms & TreatmentDocument13 pagesBronchiectasis Guide: Causes, Symptoms & TreatmentshriyaNo ratings yet
- Salicylic Acid InfoDocument6 pagesSalicylic Acid InfoPépé TechopathamNo ratings yet
- Cardiac Drugs PowerpointDocument17 pagesCardiac Drugs PowerpointNoci M. FrenkNo ratings yet
- CASE REPORT ON MYOMA UTERINEDocument12 pagesCASE REPORT ON MYOMA UTERINENiki Rizqi rachmawatiNo ratings yet
- Bacteriophages in Health and DiseaseDocument297 pagesBacteriophages in Health and DiseaseCisticola100% (1)
- RTOG Breast Cancer Atlas For Radiation Therapy PlanningDocument71 pagesRTOG Breast Cancer Atlas For Radiation Therapy Planningdoctordoctor80No ratings yet
- Notes On PsychiatryDocument10 pagesNotes On PsychiatryMark VillenaNo ratings yet
- Yellow Fever Brochure PubDocument2 pagesYellow Fever Brochure Pubapi-358102097No ratings yet
- BPH PresentationDocument33 pagesBPH PresentationKwabena AmankwaNo ratings yet
- Final SdvsDocument22 pagesFinal SdvsKesavanadh T MNo ratings yet
- Penyesuaian Dosis Regimen Pada Pasien Dengan Gangguan Fungsi GinjalDocument19 pagesPenyesuaian Dosis Regimen Pada Pasien Dengan Gangguan Fungsi GinjalChamidRiyadiNo ratings yet
- Assistant Professor in Community Dentistry - Previous PSC Question PaperDocument11 pagesAssistant Professor in Community Dentistry - Previous PSC Question PaperXaviorNo ratings yet
- Acute Effects of Radiation InjuryDocument8 pagesAcute Effects of Radiation InjuryVikas VatsNo ratings yet
- 4mat Paper #2 Hope-Focused MarriageDocument9 pages4mat Paper #2 Hope-Focused Marriagemyyahoo2No ratings yet
- Repressed Emotions: A Definitive Guide To Liberating YourselfDocument19 pagesRepressed Emotions: A Definitive Guide To Liberating Yourselfcoachbiznesu100% (1)
- PainDocument34 pagesPainFelicia ChristantyNo ratings yet
- Chelsea Schneider ResumeDocument3 pagesChelsea Schneider Resumeapi-308629385No ratings yet
- Concept of PHA 2Document7 pagesConcept of PHA 2Lekha Bahadur GurungNo ratings yet
- A Study of Cryo Stemcell Banking in Mumbai - Awareness and Acceptance by CustomerDocument45 pagesA Study of Cryo Stemcell Banking in Mumbai - Awareness and Acceptance by Customerabhijit055No ratings yet
- Intermittent Compression RubricDocument2 pagesIntermittent Compression RubricSteve ColbertNo ratings yet
- Pharmacology Quizlet: Chapter 1 Intro To PharmacologyDocument18 pagesPharmacology Quizlet: Chapter 1 Intro To PharmacologyJerome ValerianoNo ratings yet
- Passage 2Document2 pagesPassage 2Minh ThanhNo ratings yet
- SkeletaxrayDocument144 pagesSkeletaxrayradiologgNo ratings yet
- Guidance Counselling BasicsDocument26 pagesGuidance Counselling BasicsNur Izzati Adam100% (4)
- Management of Ruptured Liver Abscess: A Study of 54 CasesDocument4 pagesManagement of Ruptured Liver Abscess: A Study of 54 CasesIndah FebrianaNo ratings yet
- 2017 Onslow Livro Stuttering and Its TreatmentDocument278 pages2017 Onslow Livro Stuttering and Its TreatmentCarol PaesNo ratings yet
- Davis Drug Guide DIU - 2016 - CombinedDocument94 pagesDavis Drug Guide DIU - 2016 - Combinedi_nurse100% (2)
- Anticoagulant Pocket GuideDocument8 pagesAnticoagulant Pocket GuideDrew John Minardi100% (2)
- Usa 19 EndDocument33 pagesUsa 19 Endrabiya100% (2)
- Clinical Practice Guideline PDFDocument351 pagesClinical Practice Guideline PDFGisela Cristina MendesNo ratings yet