You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Abnormal EcgDocument8 pagesAbnormal EcgM.DalaniNo ratings yet
- Nifedipine-Drug Study 2BSN3Document3 pagesNifedipine-Drug Study 2BSN3Nichole DancelNo ratings yet
- Nursing Seminar 1 SAS Session 21Document9 pagesNursing Seminar 1 SAS Session 21ZiaNo ratings yet
- Cms Files 3250 1447504505Saúde+-+Cardiovascular+Risk+Falls+in+Patients+With+Rheumatoid+ArthritisDocument3 pagesCms Files 3250 1447504505Saúde+-+Cardiovascular+Risk+Falls+in+Patients+With+Rheumatoid+ArthritisTuba ArtelloNo ratings yet
- Tetralogy of Fallot.......Document7 pagesTetralogy of Fallot.......Sam AlipioNo ratings yet
- CareofolderadultsDocument8 pagesCareofolderadultsMonique FranciscoNo ratings yet
- ACLS ACS Algorithm NewDocument3 pagesACLS ACS Algorithm Newsambo100% (1)
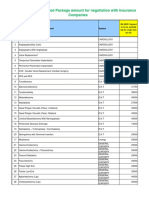
- IMA NHB Suggested Package Amount For Negotiation With Insurance CompaniesDocument5 pagesIMA NHB Suggested Package Amount For Negotiation With Insurance Companiesmonikparmar1No ratings yet
- Katalog Journals and Book Series 2023 DigitalDocument165 pagesKatalog Journals and Book Series 2023 DigitalMuhammad AliNo ratings yet
- Accelerated Idioventricular RhythmDocument5 pagesAccelerated Idioventricular RhythmMed AmineNo ratings yet
- A Clinical Approach To SyncopeDocument8 pagesA Clinical Approach To Syncopepuskesmas tarik100% (1)
- Cardiovascular Examination:: General InspectionDocument6 pagesCardiovascular Examination:: General InspectionPhysician AssociateNo ratings yet
- Transposition of The Great ArteriesDocument17 pagesTransposition of The Great ArteriesGaram Esther GohNo ratings yet
- Electrocardiogram - Wikipedia, The Free EncyclopediaDocument16 pagesElectrocardiogram - Wikipedia, The Free EncyclopediaRaJeev K SookunNo ratings yet
- Ecg Level 3 Precise Calculation of Cardiac AxisDocument44 pagesEcg Level 3 Precise Calculation of Cardiac Axismoneer chanceNo ratings yet
- Cardiovascular SystemDocument624 pagesCardiovascular Systempattumkp100% (1)
- Cardiovascular & Neurology Update 2023Document1 pageCardiovascular & Neurology Update 2023Christian TariganNo ratings yet
- Intensive Care Unit (ICU)Document6 pagesIntensive Care Unit (ICU)Joanne Bernadette AguilarNo ratings yet
- DHQ Internship ReportDocument49 pagesDHQ Internship ReportRana HaseebNo ratings yet
- Sudden Cardiac Death in Young AthletesDocument6 pagesSudden Cardiac Death in Young AthletesnulintavaNo ratings yet
- ECG InterpretationDocument82 pagesECG InterpretationIin Widya Sari Siregar100% (1)
- Empanelled Hospitals CGHSDocument107 pagesEmpanelled Hospitals CGHSankit.shrivastavaNo ratings yet
- 9 CsaDocument34 pages9 Csaمحمد بن الصادقNo ratings yet
- Preliminary Programme ERC2011Document12 pagesPreliminary Programme ERC2011ExpuneriMedicaleNo ratings yet
- Cardiovascular Drugs XL ChartDocument4 pagesCardiovascular Drugs XL Chartcdp158767% (3)
- Alsoufi 2018Document2 pagesAlsoufi 2018nidaakkusNo ratings yet
- Normal ECGDocument2 pagesNormal ECGGeneon100% (1)
- Scientific Programme 18th APCC 090311Document33 pagesScientific Programme 18th APCC 090311drsmiNo ratings yet
- ECG Criterias For Ventricular Hypertrophy by DR PRASANTH SDocument13 pagesECG Criterias For Ventricular Hypertrophy by DR PRASANTH SnadineNo ratings yet
- What Is Cardiac AblationDocument2 pagesWhat Is Cardiac AblationShay Patrick CormacNo ratings yet