You might also like
- Ekadashi PDFDocument30 pagesEkadashi PDFkaram0% (1)
- BC 0009 ModMethods JLD Part 2Document55 pagesBC 0009 ModMethods JLD Part 2karamNo ratings yet
- BC 0009 ModMethods JLD Part 1Document79 pagesBC 0009 ModMethods JLD Part 1karamNo ratings yet
- Qplum Fractional RebalancingDocument8 pagesQplum Fractional RebalancingkaramNo ratings yet
- The Advantage of ParliamentaryDocument29 pagesThe Advantage of ParliamentaryShan KhingNo ratings yet
- Ryan Holiday Reccomendation On Strategy Books ReadingDocument11 pagesRyan Holiday Reccomendation On Strategy Books ReadingkaramNo ratings yet
- Open Access Content MIT PressDocument8 pagesOpen Access Content MIT PresskaramNo ratings yet
- What Will Be The Cause of The Next Financial CrashDocument7 pagesWhat Will Be The Cause of The Next Financial CrashkaramNo ratings yet
- Juan Linz, Presidentialism, and Democracy PDFDocument26 pagesJuan Linz, Presidentialism, and Democracy PDFkaramNo ratings yet
- BAIN REPORT Global Healthcare Private Equity 2016 PDFDocument40 pagesBAIN REPORT Global Healthcare Private Equity 2016 PDFkaramNo ratings yet
- Tufts CSDD Briefing On RD Cost Study - Nov 18, 2014.Document30 pagesTufts CSDD Briefing On RD Cost Study - Nov 18, 2014.karamNo ratings yet
- Beers Law CalculationsDocument3 pagesBeers Law CalculationskaramNo ratings yet
- Value Based Healthcare - Porter PDFDocument34 pagesValue Based Healthcare - Porter PDFkaramNo ratings yet
- Antibody Drug Conjugates Promise and Challenges Wendy-Weinberg of FDA 01-10-11Document40 pagesAntibody Drug Conjugates Promise and Challenges Wendy-Weinberg of FDA 01-10-11karamNo ratings yet
- Framework For Case AnalysisDocument14 pagesFramework For Case AnalysisShruti DesaiNo ratings yet
- Introduction To Case StudiesDocument54 pagesIntroduction To Case StudieskaramNo ratings yet
- InseadDocument8 pagesInseadLizbeth ParedesNo ratings yet
- The Advisory Board CompanyDocument22 pagesThe Advisory Board CompanykaramNo ratings yet
- Review On The Design Art of BiosensorsDocument22 pagesReview On The Design Art of BiosensorskaramNo ratings yet
- Antibody Purification HandbookDocument171 pagesAntibody Purification HandbookOana CatinasNo ratings yet
- Handling Cytotoxic PDFDocument58 pagesHandling Cytotoxic PDFnikensantosoNo ratings yet
- Safe Handling of CytotoxicsDocument11 pagesSafe Handling of CytotoxicskaramNo ratings yet
- Framework For Case AnalysisDocument14 pagesFramework For Case AnalysisShruti DesaiNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- SSA PDC 8a&bDocument2 pagesSSA PDC 8a&bMageswary Kunalan100% (2)
- Brochure Clack Corporation - Granular Activated Carbon, 2pDocument2 pagesBrochure Clack Corporation - Granular Activated Carbon, 2pNestramiNo ratings yet
- Vitas ng Tondo documentary highlights poverty and health issuesDocument2 pagesVitas ng Tondo documentary highlights poverty and health issuesAkemi ParkNo ratings yet
- Soal Bing Xi BaruDocument5 pagesSoal Bing Xi BarumujiamanNo ratings yet
- James A. Gifford Causeway Rehabilitation UpdateDocument31 pagesJames A. Gifford Causeway Rehabilitation UpdatePeterborough ExaminerNo ratings yet
- XS-1 MSDSDocument4 pagesXS-1 MSDSgregorypage2No ratings yet
- Ben Jonson. The Masque of Blackness. 1605Document9 pagesBen Jonson. The Masque of Blackness. 1605Luri IacobNo ratings yet
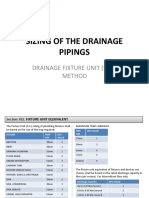
- Sizing Drainage Piping Using Fixture Unit MethodDocument7 pagesSizing Drainage Piping Using Fixture Unit Methodelcid agsamosamNo ratings yet
- Axion Dishwashing Hand Lemon-Lime 5.30.07 - ColgateDocument3 pagesAxion Dishwashing Hand Lemon-Lime 5.30.07 - ColgateBLU LOGISTICS COLOMBIANo ratings yet
- 1 - API 571 (19 DMS)Document42 pages1 - API 571 (19 DMS)Mohammed Kadhim100% (2)
- Ove 17718VN-S Huongdanlapdat PDFDocument9 pagesOve 17718VN-S Huongdanlapdat PDFTien PhamNo ratings yet
- DPT Well S & ADocument57 pagesDPT Well S & ABrahim Letaief100% (2)
- Forward Osmosis - Low Pressure Reverse Osmosis For Water Reuse (PDFDrive)Document123 pagesForward Osmosis - Low Pressure Reverse Osmosis For Water Reuse (PDFDrive)FerminNo ratings yet
- GasStop Gas Migration Control AdditiveDocument2 pagesGasStop Gas Migration Control Additivebagus918100% (1)
- Clean and Healthy IndiaDocument2 pagesClean and Healthy IndiaMeenakshi SinghNo ratings yet
- Hydrogeological Processes in Karst TerranesDocument422 pagesHydrogeological Processes in Karst TerranesAbdullah Cem Koç100% (1)
- Surface Water Treatment For InjectionDocument21 pagesSurface Water Treatment For InjectionHedi Ben MohamedNo ratings yet
- Essay Assignment - Waters Journey 1Document5 pagesEssay Assignment - Waters Journey 1api-641496664No ratings yet
- Presentation On Industrial Water Circulation SystemDocument19 pagesPresentation On Industrial Water Circulation Systembashok87No ratings yet
- Types of Construction WorkDocument6 pagesTypes of Construction WorkKalsoma CarlsNo ratings yet
- Ch1-Soil Definition & FormationDocument20 pagesCh1-Soil Definition & FormationRafi SulaimanNo ratings yet
- Hyperspectral Crop Stress Study in Mexico Reveals Potential for Precision AgricultureDocument6 pagesHyperspectral Crop Stress Study in Mexico Reveals Potential for Precision AgriculturesergonzalezNo ratings yet
- The Estuarine EcosystemDocument223 pagesThe Estuarine EcosystemRodrigo AguayoNo ratings yet
- Sheet pile cofferdam design and economic analysisDocument3 pagesSheet pile cofferdam design and economic analysisMuhammad Irfan50% (2)
- New Microsoft Office PowerPoint PresentationDocument28 pagesNew Microsoft Office PowerPoint PresentationGuleRia ShiVaniNo ratings yet
- DaVinci Safety CoversDocument3 pagesDaVinci Safety CoversFort Wayne Sterling PoolsNo ratings yet
- Laporan Cadangan PemajuanDocument22 pagesLaporan Cadangan PemajuanHasbullah SalehNo ratings yet
- QCP For Hot Tap PDFDocument30 pagesQCP For Hot Tap PDFjahaan100% (1)
- MR Lim's IDU JournalDocument19 pagesMR Lim's IDU Journal박지훈No ratings yet
- Banner Ketiga 3 FitDocument17 pagesBanner Ketiga 3 FitVishnu KrishnanNo ratings yet