You might also like
- A Cure For Cancer Hidden in Plain Sight July 2019 DR David WilliamsDocument8 pagesA Cure For Cancer Hidden in Plain Sight July 2019 DR David WilliamsThomas Van Beek100% (2)
- Canadian: Hypoglycemia: Understanding The EnemyDocument8 pagesCanadian: Hypoglycemia: Understanding The EnemyndistantiNo ratings yet
- The Rubik's Cube Approach To Clinical MedicineDocument2 pagesThe Rubik's Cube Approach To Clinical Medicinehenrygoldstein100% (1)
- Clinical Inertia in T2DM ManagementDocument11 pagesClinical Inertia in T2DM ManagementEva GabrielNo ratings yet
- ACP Insulin SlideCAST 222Document197 pagesACP Insulin SlideCAST 222charanmann9165No ratings yet
- ANNALS-Diabetes Tipo IIDocument16 pagesANNALS-Diabetes Tipo IIewb100% (2)
- Sitagliptin Slide Set Specialist - 1Document31 pagesSitagliptin Slide Set Specialist - 1Fannia Setiani100% (1)
- Prediabetes Progression and TreatmentDocument8 pagesPrediabetes Progression and TreatmentVimal NishadNo ratings yet
- Diabetes Update: Facts Show Growing Prevalence and Costs Despite Intensifying TreatmentDocument28 pagesDiabetes Update: Facts Show Growing Prevalence and Costs Despite Intensifying TreatmentPilar Victoria Arrieta VegaNo ratings yet
- Basal Bolus InsulinDMT22009Document92 pagesBasal Bolus InsulinDMT22009scribdNo ratings yet
- AIIMS (MBBS) Solved Question Paper 2010Document34 pagesAIIMS (MBBS) Solved Question Paper 2010cbsestudymaterialsNo ratings yet
- Unmet Needs in Diabetes: Present and Future From Clinical PracticeDocument53 pagesUnmet Needs in Diabetes: Present and Future From Clinical PracticescribdNo ratings yet
- Using Enzymes to Diagnose and Treat DiseasesDocument30 pagesUsing Enzymes to Diagnose and Treat DiseasesAnubhav sainiNo ratings yet
- Acp Sglt2 Slidecast 220Document169 pagesAcp Sglt2 Slidecast 220charanmann9165No ratings yet
- Glucose Control in Diabetes: Focus On SulfhonylureaDocument93 pagesGlucose Control in Diabetes: Focus On SulfhonylureascribdNo ratings yet
- Advisory Board PPT (Dr-2. Ida Ayu Kshanti SPPD, KEMD)Document29 pagesAdvisory Board PPT (Dr-2. Ida Ayu Kshanti SPPD, KEMD)scribdNo ratings yet
- tmpFF74 TMPDocument2 pagestmpFF74 TMPFrontiersNo ratings yet
- TEACHING OF DIABETES MELLITUSDocument4 pagesTEACHING OF DIABETES MELLITUSpearl_nursingNo ratings yet
- Building A Diabetes Alliance: The Role of Provider EducationDocument32 pagesBuilding A Diabetes Alliance: The Role of Provider EducationMark ReinhardtNo ratings yet
- Polypharmacy in The Aging Patient A Review of Glycemic Control in Older Adults With Type 2 DiabetesDocument12 pagesPolypharmacy in The Aging Patient A Review of Glycemic Control in Older Adults With Type 2 Diabetesapi-311409998No ratings yet
- Management of Inpatient Hyperglycemia: 2011 Endocrine Society MeetingDocument5 pagesManagement of Inpatient Hyperglycemia: 2011 Endocrine Society MeetingDirga Rasyidin LNo ratings yet
- Management of Diabetes Mellitus in Patients With Chronic Kidney DiseaseDocument9 pagesManagement of Diabetes Mellitus in Patients With Chronic Kidney DiseasezakyNo ratings yet
- Presentation Indonesia Sep 8 2022Document88 pagesPresentation Indonesia Sep 8 2022yuni chanNo ratings yet
- Hypoglycemia: The Neglected Complication: Review ArticleDocument16 pagesHypoglycemia: The Neglected Complication: Review Articlesiti nur aishah jalilNo ratings yet
- From Evidence to Clinical Practice in Diabetes ManagementDocument40 pagesFrom Evidence to Clinical Practice in Diabetes ManagementscribdNo ratings yet
- The Legacy Effect of Early Intensive Glycemic ControlDocument9 pagesThe Legacy Effect of Early Intensive Glycemic ControlSouradipta GangulyNo ratings yet
- Cardiometabolic Syndrome: & DR Dhafir A. MahmoodDocument62 pagesCardiometabolic Syndrome: & DR Dhafir A. MahmoodJacob AlphaNo ratings yet
- Diabetes Management UpdateDocument64 pagesDiabetes Management UpdatethisarNo ratings yet
- HTTPDocument65 pagesHTTPAndreea SlabuNo ratings yet
- Intensification of Insulin Therapy in Patients With Type 2 Diabetes Mellitus An Algorithm For Basal Bolus TherapyDocument12 pagesIntensification of Insulin Therapy in Patients With Type 2 Diabetes Mellitus An Algorithm For Basal Bolus TherapyYudi Fadilah100% (1)
- Research: Cite This As: BMJ 2010 341:c3337Document7 pagesResearch: Cite This As: BMJ 2010 341:c3337Deepak DahiyaNo ratings yet
- Mingrone 2015Document10 pagesMingrone 2015Ana GomezNo ratings yet
- Pathology of Type 2 DiabetesDocument4 pagesPathology of Type 2 DiabetesJenny SembranoNo ratings yet
- The Influence of Glucose Self-Monitoring On Glycaemic Control in Patients With Diabetes Mellitus in SudanDocument5 pagesThe Influence of Glucose Self-Monitoring On Glycaemic Control in Patients With Diabetes Mellitus in SudanZam-zam RsiNo ratings yet
- DPP-4 Inhibitor and The BrainDocument19 pagesDPP-4 Inhibitor and The BrainSurat TanprawateNo ratings yet
- Editorial: Preventing Diabetic Retinopathy ProgressionDocument3 pagesEditorial: Preventing Diabetic Retinopathy ProgressionRashellya RasyidaNo ratings yet
- Semaglutide 1.0 mg More Effective for Glycemic Control & Weight Loss Than Liraglutide 1.2 mgDocument10 pagesSemaglutide 1.0 mg More Effective for Glycemic Control & Weight Loss Than Liraglutide 1.2 mgIvan Dario Hernandez ErazoNo ratings yet
- 5 - Diabetes MellitusDocument9 pages5 - Diabetes MellitusNatnicha foongfaNo ratings yet
- Clinical Case Study DMDocument12 pagesClinical Case Study DMapi-370434100No ratings yet
- Diabetes Care in Indonesia - Role of GLP 1 Analog: Pradana SoewondoDocument58 pagesDiabetes Care in Indonesia - Role of GLP 1 Analog: Pradana SoewondoscribdNo ratings yet
- Ramachandran 2006Document9 pagesRamachandran 2006Dharsheena Seshadri ManogaranNo ratings yet
- Type 2 Diabetes Mellitus Disease Diagnosis and Treatment 2155 6156 1000533Document6 pagesType 2 Diabetes Mellitus Disease Diagnosis and Treatment 2155 6156 1000533Sasa AprilaNo ratings yet
- InsulinaDocument8 pagesInsulinaClaudiu SufleaNo ratings yet
- 25 OS OD: Progression of Diabetic Retinopathy in The Hypertension Intervention Nurse Telemedicine StudyDocument2 pages25 OS OD: Progression of Diabetic Retinopathy in The Hypertension Intervention Nurse Telemedicine Studyanisarahma718No ratings yet
- Hypoglycemia - The Neglected ComplicationDocument23 pagesHypoglycemia - The Neglected Complication4g5xwdvh9sNo ratings yet
- Cost-Effectiveness - A Modeled AnalysisDocument13 pagesCost-Effectiveness - A Modeled AnalysisAngelo Cardoso PereiraNo ratings yet
- Research Proposal IntroductionDocument8 pagesResearch Proposal IntroductionIsaac OmwengaNo ratings yet
- Metformin For Diabetes Prevention: Insights Gained From The Diabetes Prevention Program/Diabetes Prevention Program Outcomes StudyDocument11 pagesMetformin For Diabetes Prevention: Insights Gained From The Diabetes Prevention Program/Diabetes Prevention Program Outcomes StudyRosa Villanueva CarrascoNo ratings yet
- Insulin Pump Therapy Associated with Lower Risk of Severe HypoglycemiaDocument10 pagesInsulin Pump Therapy Associated with Lower Risk of Severe HypoglycemiaCaroline QueirogaNo ratings yet
- Evaluation of Knowledge and Self Care Practices in Diabetic Patients and Their Role in Disease ManagementDocument4 pagesEvaluation of Knowledge and Self Care Practices in Diabetic Patients and Their Role in Disease ManagementSharmela BrijmohanNo ratings yet
- Detection of Diabetic Complications by Primary Care PhysiciansDocument5 pagesDetection of Diabetic Complications by Primary Care PhysiciansAMBS ABMS JMAANo ratings yet
- AppendixDocument105 pagesAppendixrahmawati aliwarmanNo ratings yet
- Prediabetes - OKE - IDI LMGNDocument48 pagesPrediabetes - OKE - IDI LMGNruthmindosiahaanNo ratings yet
- DPP4 Inhibitors: Mechanisms and ApplicationsDocument5 pagesDPP4 Inhibitors: Mechanisms and Applicationsstorm2138No ratings yet
- Cud BdiabetesDocument10 pagesCud BdiabetesShitanjni WatiNo ratings yet
- Follow-Up of Glycemic Control andDocument17 pagesFollow-Up of Glycemic Control anddradrianramdhanyNo ratings yet
- Managing Diabetes in Primary Care in The CaribbeanDocument24 pagesManaging Diabetes in Primary Care in The CaribbeanAndre SookdarNo ratings yet
- AI researchDocument16 pagesAI researchshiringohariiiNo ratings yet
- Gestational DiabetiesDocument50 pagesGestational DiabetiesAkshat Goel100% (1)
- Exercise and Type 2 DiabetesDocument15 pagesExercise and Type 2 Diabetespb.nakulaNo ratings yet
- CPG Management of Chronic Kidney Disease in Adults June 2011Document47 pagesCPG Management of Chronic Kidney Disease in Adults June 2011Kokoland KukusNo ratings yet
- Ass Knowledge and MaDocument1 pageAss Knowledge and MaB04-BALKIS SOLEHAHNo ratings yet
- 349 FullDocument3 pages349 FullsenkonenNo ratings yet
- Diabetes Complications—Preventing Vision Loss and Kidney DiseaseDocument12 pagesDiabetes Complications—Preventing Vision Loss and Kidney DiseaseAnam MirNo ratings yet
- Management of Hyperglycaemia and Steroid (Glucocorticoid) TherapyDocument28 pagesManagement of Hyperglycaemia and Steroid (Glucocorticoid) TherapyLatifatu ChoirunisaNo ratings yet
- Meeting the American Diabetes Association Standards of Care: An Algorithmic Approach to Clinical Care of the Diabetes PatientFrom EverandMeeting the American Diabetes Association Standards of Care: An Algorithmic Approach to Clinical Care of the Diabetes PatientNo ratings yet
- Diabetes Care in Indonesia - Role of GLP 1 Analog: Pradana SoewondoDocument58 pagesDiabetes Care in Indonesia - Role of GLP 1 Analog: Pradana SoewondoscribdNo ratings yet
- Ways To Improve The Macrovascular Outcomes in Type 2 Diabetes TherapyDocument42 pagesWays To Improve The Macrovascular Outcomes in Type 2 Diabetes TherapyscribdNo ratings yet
- PDCI Core Kit 15 Indications For Referral of Complex PatientsDocument49 pagesPDCI Core Kit 15 Indications For Referral of Complex PatientsscribdNo ratings yet
- Shangri-La JKT - JDMDocument2 pagesShangri-La JKT - JDMscribdNo ratings yet
- Role of Kidney (Unmet Need in T2DM) For Prof SarwonoDocument25 pagesRole of Kidney (Unmet Need in T2DM) For Prof SarwonoscribdNo ratings yet
- Current Concepts of Chronic Diabetic ComplicationsDocument4 pagesCurrent Concepts of Chronic Diabetic ComplicationsscribdNo ratings yet
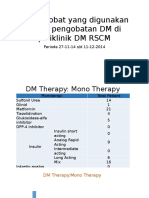
- Survey Obat DM Poli Endokrin (Prof - Sarwono)Document8 pagesSurvey Obat DM Poli Endokrin (Prof - Sarwono)scribdNo ratings yet
- Sist - Penelitian ProDocument57 pagesSist - Penelitian ProscribdNo ratings yet
- Unmet Need DM Management in Primary Care Seting 280914Document62 pagesUnmet Need DM Management in Primary Care Seting 280914scribdNo ratings yet
- Basic Metabolism Per Ho Mped in 2013Document44 pagesBasic Metabolism Per Ho Mped in 2013scribdNo ratings yet
- DMCombos JDM2014Document160 pagesDMCombos JDM2014scribdNo ratings yet
- DMcombos JDM2014Document5 pagesDMcombos JDM2014scribdNo ratings yet
- Workshop: Case StudyDocument28 pagesWorkshop: Case StudyscribdNo ratings yet
- DMB DNG 2014 Su AdvanceDocument42 pagesDMB DNG 2014 Su AdvancescribdNo ratings yet
- Metformin at the Core of T2DM TreatmentDocument37 pagesMetformin at the Core of T2DM TreatmentscribdNo ratings yet
- From Evidence to Clinical Practice in Diabetes ManagementDocument40 pagesFrom Evidence to Clinical Practice in Diabetes ManagementscribdNo ratings yet
- Data Statistik Ujian Peserta S3Document18 pagesData Statistik Ujian Peserta S3scribdNo ratings yet
- Jafes 28 01 Oa 08 AbstractDocument2 pagesJafes 28 01 Oa 08 AbstractscribdNo ratings yet
- PDCI Core Kit 15 Indications For Referral of Complex PatientsDocument49 pagesPDCI Core Kit 15 Indications For Referral of Complex PatientsscribdNo ratings yet
- DTU Slides023AcarboseDocument19 pagesDTU Slides023AcarbosescribdNo ratings yet
- Jafes 28-01-Oa-08 Eb Deliberation FormDocument1 pageJafes 28-01-Oa-08 Eb Deliberation FormscribdNo ratings yet
- Obat Rujuk BalikDocument54 pagesObat Rujuk BalikscribdNo ratings yet
- Makalah Prof Pradana Challenges in Diabetes Management in Indonesia (BioMed 2013)Document20 pagesMakalah Prof Pradana Challenges in Diabetes Management in Indonesia (BioMed 2013)scribdNo ratings yet
- Dtu Slides022ukpds PTMDocument14 pagesDtu Slides022ukpds PTMscribdNo ratings yet
- Dtu Slides004ukpdsDocument12 pagesDtu Slides004ukpdsscribdNo ratings yet
- Metabolic Problems and Vascular Disease: Sarwono WaspadjiDocument58 pagesMetabolic Problems and Vascular Disease: Sarwono WaspadjiscribdNo ratings yet
- Diagnosis and Treatment of Limb Fractures Associated With Acute Peripheral IschemiaDocument6 pagesDiagnosis and Treatment of Limb Fractures Associated With Acute Peripheral IschemiaramadhaniandaNo ratings yet
- AIIMS Dental PG November 2009 Solved Question Paper PDFDocument16 pagesAIIMS Dental PG November 2009 Solved Question Paper PDFDr-Amit PandeyaNo ratings yet
- Create PDFDocument10 pagesCreate PDFAthanasia SergouniotiNo ratings yet
- Frequency, Severity, and Distress of Dialysis-Related Symptoms Reported by Patients On HemodialysisDocument1 pageFrequency, Severity, and Distress of Dialysis-Related Symptoms Reported by Patients On HemodialysisHelvia RahayuNo ratings yet
- CT ScanDocument37 pagesCT ScanBayu Ihkshan Yamada TriatmojoNo ratings yet
- Stepwise Ventilator Waveform Assessment To Diagnose Pulmonary PathophysiologyDocument8 pagesStepwise Ventilator Waveform Assessment To Diagnose Pulmonary PathophysiologyPablo Simón Narbona MenaNo ratings yet
- Laminectomy Definition: Spine Surgery to Relieve Pressure on Spinal Cord or NervesDocument9 pagesLaminectomy Definition: Spine Surgery to Relieve Pressure on Spinal Cord or NervesEdmarie AmistadNo ratings yet
- Demand For Beauty by Society (FINAL)Document10 pagesDemand For Beauty by Society (FINAL)Maryhan MukhalalatiNo ratings yet
- Addiction CaseDocument4 pagesAddiction CasePooja VarmaNo ratings yet
- Dimension EXL 200/EXL With LM Integrated Chemistry Systems: Global Test MenuDocument2 pagesDimension EXL 200/EXL With LM Integrated Chemistry Systems: Global Test MenuGuneyden GuneydenNo ratings yet
- Free Journal List For PublicationDocument11 pagesFree Journal List For PublicationSyed Saad AliNo ratings yet
- The Journal of Rheumatology Volume 42, No. 7Document7 pagesThe Journal of Rheumatology Volume 42, No. 7salclNo ratings yet
- TTTTDocument26 pagesTTTTMoataz TrabehNo ratings yet
- What is GastroschisisDocument6 pagesWhat is GastroschisisAnonymous MWd5UOUuiyNo ratings yet
- Neurofeedback Technician or Psychotherapist or Career CounselorDocument3 pagesNeurofeedback Technician or Psychotherapist or Career Counselorapi-121357186No ratings yet
- EHAQ 4th Cycle Audit Tool Final Feb.10-2022Document51 pagesEHAQ 4th Cycle Audit Tool Final Feb.10-2022Michael Gebreamlak100% (1)
- Mandala Coloring For Children With Symptoms of Attention Deficit Hyperactivity Disorder - A Case SeriesDocument7 pagesMandala Coloring For Children With Symptoms of Attention Deficit Hyperactivity Disorder - A Case Seriesindex PubNo ratings yet
- PPM Action Plan - 13 - 01 - 2022Document128 pagesPPM Action Plan - 13 - 01 - 2022whoosh2008No ratings yet
- CasopisiDocument452 pagesCasopisiGormi DurmiNo ratings yet
- Global epidemiology of periodontal diseaseDocument16 pagesGlobal epidemiology of periodontal diseaseBrenda Carolina Pattigno ForeroNo ratings yet
- Dialog Roleplay Bahasa Inggris: Disusun Oleh Kelompok 3Document4 pagesDialog Roleplay Bahasa Inggris: Disusun Oleh Kelompok 3Desma LindaNo ratings yet
- Cpe Common Diagnoses 6-4-2021Document9 pagesCpe Common Diagnoses 6-4-2021Shubham HarishNo ratings yet
- Platelet Rich FibrinDocument7 pagesPlatelet Rich FibrinNelly AndriescuNo ratings yet
- MSB Viewing Guide - 0102Document4 pagesMSB Viewing Guide - 0102Jess WestwoodNo ratings yet
- ImmerciDocument14 pagesImmercitextilessathishNo ratings yet
- High Output Renal FailureDocument4 pagesHigh Output Renal Failuredrhiwaomer100% (1)