You might also like
- Full Surgery Summary DONEDocument69 pagesFull Surgery Summary DONEAmalNo ratings yet
- P Wave T Waves QRS ComplexDocument16 pagesP Wave T Waves QRS ComplexYousef Al-AmeenNo ratings yet
- Liver FailureDocument2 pagesLiver Failuredude dNo ratings yet
- Elixir June 1st Week-Top10MostDifficultQuestionsDocument6 pagesElixir June 1st Week-Top10MostDifficultQuestionsadiNo ratings yet
- Acute Pancreatitis by DR DilmoDocument50 pagesAcute Pancreatitis by DR Dilmosinan kNo ratings yet
- Surgery Class Biliary System SurgeryDocument69 pagesSurgery Class Biliary System SurgeryKashif BurkiNo ratings yet
- Plab-1 1700 MCQs Solved With Explanation (Shared by Ussama Maqbool)Document729 pagesPlab-1 1700 MCQs Solved With Explanation (Shared by Ussama Maqbool)Omar Abo el nagaNo ratings yet
- Coll. - Tips and Tricks For PLABDocument174 pagesColl. - Tips and Tricks For PLABdrshekarforyouNo ratings yet
- Dr. S.P. Hewawasam (MD) Consultant Gastroenterologist/Senior Lecturer in PhysiologyDocument33 pagesDr. S.P. Hewawasam (MD) Consultant Gastroenterologist/Senior Lecturer in PhysiologyAjung SatriadiNo ratings yet
- Anaesthesia in Emergency Laparotomy: Speaker:P.Shravani Moderator:Dr.K.Vinay Assistant ProfessorDocument52 pagesAnaesthesia in Emergency Laparotomy: Speaker:P.Shravani Moderator:Dr.K.Vinay Assistant ProfessorSanthi Swetha PudhotaNo ratings yet
- Superior Vena Cava Obstruction-Raised ICP-BleedingDocument31 pagesSuperior Vena Cava Obstruction-Raised ICP-BleedingSA NodeNo ratings yet
- PancreatitisDocument59 pagesPancreatitisAarif RanaNo ratings yet
- On Co EmergenciesDocument6 pagesOn Co EmergenciessdfNo ratings yet
- Initial Trauma MusculoskeletalDocument53 pagesInitial Trauma MusculoskeletalAnonymous wyBvCzkENo ratings yet
- CholangitisDocument4 pagesCholangitisNarianne Mae Solis Bedoy100% (1)
- Final MBBS 2020 March Medicine Review KelaniyaDocument22 pagesFinal MBBS 2020 March Medicine Review KelaniyaPrathibha FernandopulleNo ratings yet
- Acute Upper GIBDocument65 pagesAcute Upper GIBAbdelrahman MokhtarNo ratings yet
- Penetrating Injury: TJ Kevin DoctorDocument105 pagesPenetrating Injury: TJ Kevin DoctorTj Kevin P-DoctorNo ratings yet
- Case Presentation: Clerk Jan Christian S. Alonzo Block 1Document25 pagesCase Presentation: Clerk Jan Christian S. Alonzo Block 1Andre SenriNo ratings yet
- Abdominal TraumaDocument39 pagesAbdominal TraumaMuvenn KannanNo ratings yet
- Surgery Notes Yr 4Document31 pagesSurgery Notes Yr 4Razeen RiyasatNo ratings yet
- Liver CirrhosisDocument9 pagesLiver CirrhosismedsmracelisNo ratings yet
- DR Fiona Dignan - Acute Haematological EmergenciesDocument37 pagesDR Fiona Dignan - Acute Haematological EmergenciesAndreKrisleeNo ratings yet
- Liver TraumaDocument7 pagesLiver TraumanouradreamNo ratings yet
- Oncology EmergencyDocument41 pagesOncology EmergencyYoussef Refaat RaoofNo ratings yet
- Clinical Clerk Seminar Series: Approach To Gi BleedsDocument11 pagesClinical Clerk Seminar Series: Approach To Gi BleedsAngel_Liboon_388No ratings yet
- PANCREASDocument74 pagesPANCREASzaiba0786No ratings yet
- CCCCCCCCCCCCCCCCCCCCCCCCCC C C ÷Document6 pagesCCCCCCCCCCCCCCCCCCCCCCCCCC C C ÷shaikameermalikNo ratings yet
- Acute PancreatitisDocument48 pagesAcute PancreatitisapocruNo ratings yet
- Abdominal TraumaDocument29 pagesAbdominal TraumaKai XinNo ratings yet
- SurgeryDocument30 pagesSurgeryLuai Tuma KhouryNo ratings yet
- 440 - Med Surg HESI 2Document8 pages440 - Med Surg HESI 2Chalcey Polson87% (15)
- Surgery 2014.1Document25 pagesSurgery 2014.1Jayanti Neogi SardarNo ratings yet
- Acute Pancreatitis (Acute Pancreatic Necrosis)Document12 pagesAcute Pancreatitis (Acute Pancreatic Necrosis)Amol DhopteNo ratings yet
- Ccemt P NotesDocument35 pagesCcemt P NotesMike LydenNo ratings yet
- Pancreatic PathologyDocument7 pagesPancreatic Pathologyzeroun24100% (1)
- Gastric Emergencies: Principles of Critical Care ModuleDocument32 pagesGastric Emergencies: Principles of Critical Care ModuleDeni AdriansyahNo ratings yet
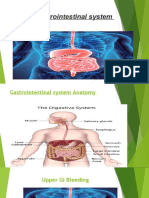
- Gastrointestinal SystemDocument26 pagesGastrointestinal SystemYazan HabaibyNo ratings yet
- RevisionLevel 3 SectionB MedSurge Case Study2Document113 pagesRevisionLevel 3 SectionB MedSurge Case Study2Milagros FloritaNo ratings yet
- Case 12669Document15 pagesCase 12669Putrisuci AndytichaNo ratings yet
- Solution Manual For Understanding The Essentials of Critical Care Nursing 0131722107Document25 pagesSolution Manual For Understanding The Essentials of Critical Care Nursing 0131722107KarenHancockwksgm100% (48)
- O Develop Either Into Hepatocytes or Intrahepatic Ductal CellsDocument10 pagesO Develop Either Into Hepatocytes or Intrahepatic Ductal CellsClint MorrisonNo ratings yet
- Banchi Final VTEDocument93 pagesBanchi Final VTEBanchiamlak AbieNo ratings yet
- What Is An Acute AbdomenDocument112 pagesWhat Is An Acute AbdomenLavasa SharmaNo ratings yet
- Trauma Pancreas ManagementDocument20 pagesTrauma Pancreas Managementazis aimaduddinNo ratings yet
- Hematemesis, Melena, HematoscheziaDocument48 pagesHematemesis, Melena, HematoscheziaSyarifah FauziahNo ratings yet
- Parathyroid Gland and Other Endocrine GlandsDocument35 pagesParathyroid Gland and Other Endocrine GlandsDrRahma Ali HeissNo ratings yet
- Pemicu 5Document75 pagesPemicu 5Cantika Monica LonanNo ratings yet
- Master File 2003 - Body As A WholeDocument32 pagesMaster File 2003 - Body As A Wholeobinna12No ratings yet
- Upper Gastrointestinal Bleeding 2007Document43 pagesUpper Gastrointestinal Bleeding 2007Matthew ThompsonNo ratings yet
- CPC Edit RMDocument39 pagesCPC Edit RMSoumya GuptaNo ratings yet
- Tehreem - Recalls MODIFIED BY Me & AARAVDocument58 pagesTehreem - Recalls MODIFIED BY Me & AARAVRohini SelvarajahNo ratings yet
- Reviewer MSDocument48 pagesReviewer MSMarithe AberosNo ratings yet
- G.I. Bleeding: Dr. Diah Ari Safitri, SPPDDocument15 pagesG.I. Bleeding: Dr. Diah Ari Safitri, SPPDmkafabillahNo ratings yet
- PM2020 I+NephrologyDocument201 pagesPM2020 I+Nephrologychongyu888xiongNo ratings yet
- Mksap NotesDocument7 pagesMksap Notesyanks1120No ratings yet
- Surgery MCQsDocument24 pagesSurgery MCQsKiara Govender100% (2)
- PSM - ImagesDocument69 pagesPSM - ImagesAbhishiktaAbhiNo ratings yet
- Netter's Atlas of Human Anatomy PDFDocument927 pagesNetter's Atlas of Human Anatomy PDFadjarra87% (46)
- Cardiology Flash Cards (EKG in A Nut Shell)Document62 pagesCardiology Flash Cards (EKG in A Nut Shell)Nabeel Kouka, MD, DO, MBA, MPHNo ratings yet
- Abortion and Ectopic PregnancyDocument145 pagesAbortion and Ectopic PregnancyAbhishiktaAbhiNo ratings yet
- GDMDocument38 pagesGDMAbhishiktaAbhi100% (1)
- Kawasaki Disease2017Document51 pagesKawasaki Disease2017AbhishiktaAbhiNo ratings yet
- 2.physiology of Reproduction in WomenDocument79 pages2.physiology of Reproduction in WomenAbhishiktaAbhiNo ratings yet
- Plab 1Document13 pagesPlab 1AbhishiktaAbhiNo ratings yet
- Final PhysicalDocument409 pagesFinal PhysicalAbhishiktaAbhiNo ratings yet
- Basic Notes by Kamal KVDocument320 pagesBasic Notes by Kamal KVRahul All73% (11)
- 1Document4 pages1AbhishiktaAbhiNo ratings yet
- MCQ Explainatory Answer: According To TNM Criteria, T2: Tumor 2 CM But 5 CM inDocument3 pagesMCQ Explainatory Answer: According To TNM Criteria, T2: Tumor 2 CM But 5 CM inAbhishiktaAbhiNo ratings yet
- Labor & Delivery Lecture Student Version FinalDocument67 pagesLabor & Delivery Lecture Student Version FinalSiti Nadzirah Mohd MayudinNo ratings yet
- 3级词汇Document1 page3级词汇AbhishiktaAbhiNo ratings yet
- HSK Vocabulaire en Karakters Niveau 3Document9 pagesHSK Vocabulaire en Karakters Niveau 3AbhishiktaAbhiNo ratings yet
- MCQ Explainatory Answer: According To TNM Criteria, T2: Tumor 2 CM But 5 CM inDocument3 pagesMCQ Explainatory Answer: According To TNM Criteria, T2: Tumor 2 CM But 5 CM inAbhishiktaAbhiNo ratings yet
- GitDocument2 pagesGitAbhishiktaAbhiNo ratings yet
- Nausea Vomiting 24Document41 pagesNausea Vomiting 24AbhishiktaAbhiNo ratings yet
- JaundiceDocument53 pagesJaundiceAbhishiktaAbhiNo ratings yet
- Chemlab 7 RenalfunctionDocument14 pagesChemlab 7 RenalfunctionAbhishiktaAbhiNo ratings yet
- Abdominal Pain31Document47 pagesAbdominal Pain31AbhishiktaAbhiNo ratings yet
- Methods of Physical ExaminationDocument41 pagesMethods of Physical ExaminationAbhishiktaAbhi100% (1)
- Urinalysis 150313040235 Conversion Gate01Document30 pagesUrinalysis 150313040235 Conversion Gate01AbhishiktaAbhi100% (1)
- BiochemistryDocument14 pagesBiochemistryAbhishiktaAbhiNo ratings yet
- 4.the AbdomenDocument82 pages4.the AbdomenAbhishiktaAbhiNo ratings yet
- Chemlab 7 RenalfunctionDocument14 pagesChemlab 7 RenalfunctionAbhishiktaAbhiNo ratings yet
- Cardiology Flash Cards (EKG in A Nut Shell)Document62 pagesCardiology Flash Cards (EKG in A Nut Shell)Nabeel Kouka, MD, DO, MBA, MPHNo ratings yet
- Exercise 2Document45 pagesExercise 2AbhishiktaAbhiNo ratings yet
- Chapter 1 General OverviewDocument43 pagesChapter 1 General OverviewAbhishiktaAbhiNo ratings yet
- Full Site PDFDocument23 pagesFull Site PDFpursuwNo ratings yet
- Testo-Flue Gas in Industry 3-27-2008Document149 pagesTesto-Flue Gas in Industry 3-27-2008leruaitesNo ratings yet
- Carpentry 7&8 Quarter 4-Module 1.2Document8 pagesCarpentry 7&8 Quarter 4-Module 1.2Mark Laurence EchaluceNo ratings yet
- UCSP Module 4Document20 pagesUCSP Module 4Agas FamilyNo ratings yet
- TMJDocument38 pagesTMJAnonymous 6kAmeZzINo ratings yet
- Aspirating Smoke Detector: Technical DescriptionDocument115 pagesAspirating Smoke Detector: Technical DescriptionSecuriton ArgentinaNo ratings yet
- Thermal Analysis of Polymers - 2008 - Menczel - FrontmatterDocument8 pagesThermal Analysis of Polymers - 2008 - Menczel - FrontmatterBABLI GUPTANo ratings yet
- Danas Si Moja I BozijaDocument1 pageDanas Si Moja I BozijaMoj DikoNo ratings yet
- Hibon - SN Ingersoll Rand BlowerDocument7 pagesHibon - SN Ingersoll Rand BlowermarquezsiemNo ratings yet
- Therelek - Heat Treatment ServicesDocument8 pagesTherelek - Heat Treatment ServicesTherelek EngineersNo ratings yet
- Low - Pass FilterDocument8 pagesLow - Pass FilterSaurabh BhiseNo ratings yet
- 9500 MPR Wireless TransmissionDocument46 pages9500 MPR Wireless TransmissionMahdi AhmadiNo ratings yet
- Immunology 2Document50 pagesImmunology 2niripsaNo ratings yet
- YES-O Action-Plan - 2022-2023Document2 pagesYES-O Action-Plan - 2022-2023carmina duldulao100% (6)
- American National Standard Safety Signs: ANSI Z535.1-2016Document42 pagesAmerican National Standard Safety Signs: ANSI Z535.1-2016Luis Enrique GonzalesNo ratings yet
- Web Based Bus Tracking SystemDocument4 pagesWeb Based Bus Tracking SystemKrishna EelaNo ratings yet
- Excess Fluid VolumeDocument27 pagesExcess Fluid VolumeAdrian Ardamil100% (1)
- Accesorios Del Lamborghini VenenoDocument31 pagesAccesorios Del Lamborghini VenenoVicente Gil PalopNo ratings yet
- Ded Deliverable List: As Per 19-08-2016Document2 pagesDed Deliverable List: As Per 19-08-2016Isna MuthoharohNo ratings yet
- Lenskart Solutions PVT LTD Company ProfileDocument13 pagesLenskart Solutions PVT LTD Company ProfileAnujaNo ratings yet
- CTL Project Developer Perspective Coal - To - Liquids CoalitionDocument27 pagesCTL Project Developer Perspective Coal - To - Liquids Coalitiondwivediashish2No ratings yet
- Igcse ReadingDocument4 pagesIgcse ReadingIvonne PuspakencanaNo ratings yet
- HorticultureDocument12 pagesHorticultureवरुण राठीNo ratings yet
- At Your Service: Affordable LandscapingDocument1 pageAt Your Service: Affordable LandscapingDamaris HigginsNo ratings yet
- Odd Semester Time Table Aug - Dec22 Wef 22.08.2022.NEWDocument4 pagesOdd Semester Time Table Aug - Dec22 Wef 22.08.2022.NEWKiran KumarNo ratings yet
- Sediments and Sedimentary Rock-Week 4Document61 pagesSediments and Sedimentary Rock-Week 4qomaruzzaman5740No ratings yet
- SUNANDA Hack Aid Plast SPL PDFDocument2 pagesSUNANDA Hack Aid Plast SPL PDFSheezan KhanNo ratings yet
- Al Khudari Company Profile FP PDFDocument14 pagesAl Khudari Company Profile FP PDFAnonymous bgYdp4No ratings yet
- Latihan Soal Report TextDocument28 pagesLatihan Soal Report TextHidayatul HikmahNo ratings yet
- Fact Sheeton Canola OilDocument15 pagesFact Sheeton Canola OilMonika ThadeaNo ratings yet