You might also like
- A Simple Guide to Skin Fungal Infections, (Updated 2023) Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Skin Fungal Infections, (Updated 2023) Diagnosis, Treatment and Related ConditionsRating: 5 out of 5 stars5/5 (2)
- Diabetic FootDocument188 pagesDiabetic FootSushil VijayNo ratings yet
- Management of Diabetic Foot Ulcers: Pandji MulyonoDocument51 pagesManagement of Diabetic Foot Ulcers: Pandji MulyonoJeffrey Dyer100% (1)
- Diabetic Foot Ulcer - Yandriyane Stephanie Robiady - 131621190504Document28 pagesDiabetic Foot Ulcer - Yandriyane Stephanie Robiady - 131621190504Yohelio Priawan SibuNo ratings yet
- Compartment SyndromeDocument21 pagesCompartment SyndromeMiztaloges86100% (1)
- Diabetic Foot UlcerDocument46 pagesDiabetic Foot UlcerNeermaladevi ParamasivamNo ratings yet
- Describing WoundsDocument4 pagesDescribing WoundsDidikPrasetyoSuliNo ratings yet
- Acute PancreatitisDocument7 pagesAcute PancreatitisVytheeshwaran Vedagiri100% (9)
- Digital Rectal ExaminationDocument21 pagesDigital Rectal ExaminationAndrew JoshuaNo ratings yet
- Diabetic FootDocument48 pagesDiabetic FootDr Shahzad Alam Shah100% (1)
- Compartment SyndromeDocument29 pagesCompartment SyndromeFazmial UjirNo ratings yet
- Case Study 4 - Neck PainDocument7 pagesCase Study 4 - Neck PainElizabeth Ho100% (1)
- Scrotal SwellingDocument63 pagesScrotal SwellingTommysNo ratings yet
- Pressure UlcerDocument35 pagesPressure Ulcerenam professor100% (1)
- Compartment SyndromeDocument36 pagesCompartment SyndromeHaziq MarsNo ratings yet
- Osteoporosis: Hani Abu DiehDocument24 pagesOsteoporosis: Hani Abu DiehAngelic khan100% (1)
- Diabetic FootDocument28 pagesDiabetic FootPrisca Yuliani SubanNo ratings yet
- Abdominal Compartment SyndromeDocument24 pagesAbdominal Compartment SyndromePrateek Vaswani100% (1)
- AMPUTATIONSDocument27 pagesAMPUTATIONSMuhammad Azhar Qureshi100% (2)
- Gastrointestinal EndosDocument28 pagesGastrointestinal EndosAqeel AhmedNo ratings yet
- Study On Pressure UlcerDocument219 pagesStudy On Pressure UlcerThein Ko Oo100% (1)
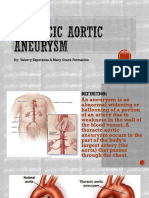
- Thoracic Aortic AneurysmDocument17 pagesThoracic Aortic AneurysmGlyssa CabarrubiasNo ratings yet
- Lecture Contents: Definitions Composition of Hernia Managment of HerniaDocument26 pagesLecture Contents: Definitions Composition of Hernia Managment of Herniaissam_1994No ratings yet
- Enterocutaneous FistulaDocument52 pagesEnterocutaneous FistulawabalyNo ratings yet
- Deep Vein ThrombosisDocument16 pagesDeep Vein ThrombosisHarinesh JayNo ratings yet
- Digital Rectal ExaminationDocument21 pagesDigital Rectal Examinationmegahed7320000No ratings yet
- HERNIORRHAPHYDocument2 pagesHERNIORRHAPHYSheldon Deypalubos Jr.No ratings yet
- Post Op Assessment SurgeryDocument20 pagesPost Op Assessment SurgeryAbdullah MatarNo ratings yet
- Esophageal CancerDocument23 pagesEsophageal Cancerabhandlung100% (3)
- Acute Urinary RetentionDocument14 pagesAcute Urinary RetentionTP RMadNo ratings yet
- BPH and Urethral StrictureDocument25 pagesBPH and Urethral Stricturezaminazz100% (1)
- Case Report Osteogenesis ImperfectaDocument52 pagesCase Report Osteogenesis ImperfectaFedelis Danii PurnawanNo ratings yet
- Fracture of Tibia and FibulaDocument31 pagesFracture of Tibia and Fibulaunknown unknown100% (1)
- Pelvic InjuriesDocument35 pagesPelvic InjuriesJavier Saad100% (1)
- Urolithiasis (Renal Calculi)Document12 pagesUrolithiasis (Renal Calculi)jhodane100% (1)
- Osteomyelitis: M.Rasoolinejad, MDDocument48 pagesOsteomyelitis: M.Rasoolinejad, MDRobert MedinaNo ratings yet
- Common Surgical Procedures TerminologyDocument10 pagesCommon Surgical Procedures TerminologySara Tongcua TacsagonNo ratings yet
- Pathophysiology of Varicose Vein - Chronic Venous InsufficiencyDocument31 pagesPathophysiology of Varicose Vein - Chronic Venous InsufficiencyDavid Christian100% (1)
- ThyroidectomyDocument5 pagesThyroidectomyJennelyn LumbreNo ratings yet
- Wound Debridement-FinalDocument3 pagesWound Debridement-FinaljessicagrepoNo ratings yet
- Wound CareDocument41 pagesWound Carekamardin zakuani100% (2)
- Peripheral Vascular DiseasesDocument72 pagesPeripheral Vascular DiseasesAnthony Riggs100% (1)
- Pelvic FracturesDocument32 pagesPelvic FracturesAgeng BudianantiNo ratings yet
- Colorectal CancerDocument29 pagesColorectal CancerLeeyanBhadzzVagayNo ratings yet
- Prostatectomy: Surgical Prostate Gland Tumour Urine UrethraDocument36 pagesProstatectomy: Surgical Prostate Gland Tumour Urine Urethranosebleed_ms3691100% (1)
- Lower GI Bleeding SlideDocument29 pagesLower GI Bleeding Slideraed faisalNo ratings yet
- SurgeryDocument12 pagesSurgeryManusheeNo ratings yet
- Peripheral Vascular DiseaseDocument36 pagesPeripheral Vascular DiseaseKeishla M Rios CardonaNo ratings yet
- What Happens in The Operating RoomDocument137 pagesWhat Happens in The Operating RoomMelchor Felipe Salvosa100% (1)
- Abdominal Aortic AneurysmDocument2 pagesAbdominal Aortic AneurysmSuhailah Mohd JamilNo ratings yet
- Cesarean Section HennawyDocument89 pagesCesarean Section Hennawykhadzx100% (2)
- Chronic Limb IschemiaDocument45 pagesChronic Limb IschemiaChristine TeNo ratings yet
- History Taking in OrthopaedicsDocument29 pagesHistory Taking in Orthopaedicsdocivirus100% (1)
- Renal CalculiDocument30 pagesRenal CalculiAnaiah Jaaziel KhanNo ratings yet
- Diabetic FoootDocument34 pagesDiabetic Foootsiakonihmat433No ratings yet
- Diabetic Foot Ulcer: By: FauzanadliDocument43 pagesDiabetic Foot Ulcer: By: FauzanadliWan RahimahNo ratings yet
- Pertanyaan CaseDocument4 pagesPertanyaan CaseAndinnyaCesaliaNo ratings yet
- Diabetic Foot: How Do The Pathophysiological Features of Diabetes Put The Foot at Increased Risk For Tissue Damage?Document8 pagesDiabetic Foot: How Do The Pathophysiological Features of Diabetes Put The Foot at Increased Risk For Tissue Damage?Kat BausaNo ratings yet
- 11 Diabetic FootDocument37 pages11 Diabetic Footkim suhoNo ratings yet
- Diabetic Foot InfectionsDocument28 pagesDiabetic Foot InfectionsFirdausAjiNo ratings yet
- New Disability Assessment Gazzette - 2024Document413 pagesNew Disability Assessment Gazzette - 2024nikkiNo ratings yet
- Diabetic Foot Assessment PDFDocument7 pagesDiabetic Foot Assessment PDFIrma KurniawatiNo ratings yet
- The Insensate FootDocument23 pagesThe Insensate FootSamedy SrorsNo ratings yet
- AAOS Foot & Ankle 2015Document114 pagesAAOS Foot & Ankle 2015Fasa Roshada100% (3)
- Diabetic Foot CareDocument50 pagesDiabetic Foot CareaswiniNo ratings yet
- Diabeticfootulcer Surgicalwounds 190908030737Document22 pagesDiabeticfootulcer Surgicalwounds 190908030737Jeevan VelanNo ratings yet
- Diabetes Foot Screen: - Can't Feel The 5.07 FilamentDocument4 pagesDiabetes Foot Screen: - Can't Feel The 5.07 FilamentSteve ChipmanNo ratings yet
- Prevention and Management of Diabetic Foot Ulcers PDFDocument68 pagesPrevention and Management of Diabetic Foot Ulcers PDFJianhua Shi100% (2)
- Frykberg RG, Et Al. Diabetic Foot Disorders.Document68 pagesFrykberg RG, Et Al. Diabetic Foot Disorders.Jared MalanNo ratings yet
- Eponymous Fractures 1Document351 pagesEponymous Fractures 1Sllavko K. Kallfa100% (2)
- Article 2Document9 pagesArticle 2105070201111009No ratings yet
- The Diabetic Foot: Current Problems in SurgeryDocument30 pagesThe Diabetic Foot: Current Problems in SurgerymarrrgNo ratings yet
- The Diagnosis of Charcot Foot: Lee C. Rogers, DPM, Nicholas J. Bevilacqua, DPMDocument9 pagesThe Diagnosis of Charcot Foot: Lee C. Rogers, DPM, Nicholas J. Bevilacqua, DPMAnonymous kdBDppigENo ratings yet
- Diabetic Foot JAAOSDocument8 pagesDiabetic Foot JAAOSAtikah ZuraNo ratings yet
- SAMY MSK ArthritisDocument125 pagesSAMY MSK ArthritisZintan HospitalNo ratings yet
- Management of Charcot JointDocument30 pagesManagement of Charcot JointdiamondNo ratings yet
- Orthobullets Foot and AnkleDocument88 pagesOrthobullets Foot and AnkleStevent Richardo100% (1)
- Osteomielitis PDFDocument14 pagesOsteomielitis PDFAngela TorresNo ratings yet
- 3 Minute Exam DFSDocument2 pages3 Minute Exam DFSWeeChuan NgNo ratings yet
- Operative Techniques in Foot and Ankle Surgery - (Axial Screw Technique For Midfoot Arthrodesis in Charcot Foot Deformit... )Document7 pagesOperative Techniques in Foot and Ankle Surgery - (Axial Screw Technique For Midfoot Arthrodesis in Charcot Foot Deformit... )Tyler Lawrence CoyeNo ratings yet
- Diabetic Foot UlcerDocument44 pagesDiabetic Foot UlcerCandy Lee100% (1)
- Diabetic Foot: The Orthopedic Surgery Angle:, T. Leemrijse, P.-A. DeleuDocument16 pagesDiabetic Foot: The Orthopedic Surgery Angle:, T. Leemrijse, P.-A. DeleuDewi Sartika100% (1)
- Dr. Amit Gupta Associate Professor Dept of SurgeryDocument43 pagesDr. Amit Gupta Associate Professor Dept of SurgeryRomauli SitorusNo ratings yet
- Extra ExtraDocument24 pagesExtra ExtrabaoNo ratings yet
- MonoarthritisDocument7 pagesMonoarthritisSalsa NadillaNo ratings yet
- Charcot Neuropathy TBH PresentationDocument15 pagesCharcot Neuropathy TBH PresentationHuguette Marie NseleNo ratings yet
- MedscapeDocument26 pagesMedscapesiti israwatiNo ratings yet
- Oite - 1998Document164 pagesOite - 1998ICH KhuyNo ratings yet
- Estate of Dennis Choquette v. Corrections Corporation of America, Et. Al.Document70 pagesEstate of Dennis Choquette v. Corrections Corporation of America, Et. Al.Michael_Lee_RobertsNo ratings yet