You might also like
- Luluh Paru (Destroyed Lung)Document3 pagesLuluh Paru (Destroyed Lung)faradilla savitriNo ratings yet
- Setting Breathing Circuits Ventilator, by RochiatiDocument37 pagesSetting Breathing Circuits Ventilator, by RochiatiAnonymous G3Av8nD100% (5)
- Konsep EWS Di RSDocument50 pagesKonsep EWS Di RSkencaNo ratings yet
- Ewss Yudi PJT RSCM PDFDocument60 pagesEwss Yudi PJT RSCM PDFRero CitroNo ratings yet
- Senam LafiskaDocument6 pagesSenam LafiskaAyuNo ratings yet
- I. Similar To Rounded Abdomen Only Greater. Anticipated in Pregnancy, Also Seen in Obesity, Ascites, and Other Conditions IIDocument3 pagesI. Similar To Rounded Abdomen Only Greater. Anticipated in Pregnancy, Also Seen in Obesity, Ascites, and Other Conditions IIroxanneNo ratings yet
- Contoh Soal Residen CardioDocument13 pagesContoh Soal Residen CardioLusyAlwiNo ratings yet
- Asma Management 08 - 09 - 07Document81 pagesAsma Management 08 - 09 - 07botolkecapNo ratings yet
- EmpyemaDocument17 pagesEmpyemadeo_gratias14No ratings yet
- Acute/Adulth Respiratory Distress Syndrome (ARDS) : RohmanDocument54 pagesAcute/Adulth Respiratory Distress Syndrome (ARDS) : RohmanMuhammad Rizki Junaidi SaputraNo ratings yet
- Indikator Saturasi OksigenDocument1 pageIndikator Saturasi OksigenAulinaNo ratings yet
- Kriteria Intubasi Dan EkstubasiDocument31 pagesKriteria Intubasi Dan Ekstubasifml grNo ratings yet
- Disaster Management of Indonesia - Kuliah Blok KedkomDocument39 pagesDisaster Management of Indonesia - Kuliah Blok KedkomNovi SeptianiNo ratings yet
- Anatomi Dan Histologi Saluran Cerna BawahDocument20 pagesAnatomi Dan Histologi Saluran Cerna BawahIlhamDevirxaNo ratings yet
- Labioschizis Dan Palatoskisis Persentasi Kelompok 1Document17 pagesLabioschizis Dan Palatoskisis Persentasi Kelompok 1Hengky HanggaraNo ratings yet
- Hubungan Pelaksanaan Screening Test Menelan Dengan Kejadian Disfagia Pada Pasien Baru Yang Menderita Stroke AkutDocument7 pagesHubungan Pelaksanaan Screening Test Menelan Dengan Kejadian Disfagia Pada Pasien Baru Yang Menderita Stroke AkutnidaNo ratings yet
- Ileus PutriDocument17 pagesIleus PutriSukir LiboNo ratings yet
- Referat AppendicitisDocument21 pagesReferat Appendicitisyaspie100% (2)
- Continuous Infusion Rate ChartDocument2 pagesContinuous Infusion Rate ChartabeNo ratings yet
- Tampak Perselubung An Opak Inhomogen Dengan Air Bronchogra M (+) Di Lapang Tengah Paru KananDocument33 pagesTampak Perselubung An Opak Inhomogen Dengan Air Bronchogra M (+) Di Lapang Tengah Paru KananEdwin DarmawanNo ratings yet
- Abnormal Chest FindingsDocument5 pagesAbnormal Chest FindingsAbishek Prince100% (1)
- Code BlueDocument16 pagesCode Blueannisamuti10No ratings yet
- BEDAH UMUM FKUI - Penatalaksanaan ApendisitisDocument7 pagesBEDAH UMUM FKUI - Penatalaksanaan ApendisitisRifda LatifaNo ratings yet
- Terapi OksigenDocument12 pagesTerapi OksigenYohana SepthiyaNo ratings yet
- Primary Survey AssessmentDocument52 pagesPrimary Survey Assessmentlapkas donjuanNo ratings yet
- Hidayaturromi-Jurnal Ileus Obstruktif PDFDocument4 pagesHidayaturromi-Jurnal Ileus Obstruktif PDFHerman HermanNo ratings yet
- Hukum CourvoisierDocument1 pageHukum CourvoisierFahryHamkaNo ratings yet
- Bagan 3 TeoriDocument1 pageBagan 3 TeoriAgis TaufikNo ratings yet
- MATERI 2 CPD DR - GALA Materi CPDDocument28 pagesMATERI 2 CPD DR - GALA Materi CPDNaura NazifahNo ratings yet
- Infeksi NosokomialDocument29 pagesInfeksi NosokomialAlunaficha Melody KiraniaNo ratings yet
- Peran Dan Fungsi Ipcn & IpclnDocument30 pagesPeran Dan Fungsi Ipcn & IpclnIno Da ConceicaoNo ratings yet
- Indikasi Dan Kontraindikasi Dekompresi JarumDocument3 pagesIndikasi Dan Kontraindikasi Dekompresi JarumNurul AtiqahNo ratings yet
- Saga Sadewa BHDDocument52 pagesSaga Sadewa BHDCOCO HTNo ratings yet
- Interpretasi EKGDocument81 pagesInterpretasi EKGGyna MarsianaNo ratings yet
- IWL FormulaDocument2 pagesIWL FormulaRahmat Sayyid ZharfanNo ratings yet
- Manajemen Anestesi ObesitasDocument21 pagesManajemen Anestesi ObesitasAndi Wija Indrawan PangerangNo ratings yet
- 2018 Farmakoterapi Obat-Obatan Emergency v2Document90 pages2018 Farmakoterapi Obat-Obatan Emergency v2saifudinNo ratings yet
- Kuliah 3. Pengaturan Osmolalitas UrinDocument19 pagesKuliah 3. Pengaturan Osmolalitas UrinAnnisa DamayantiNo ratings yet
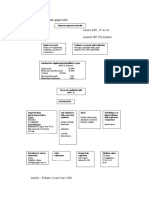
- Algoritma Penatalaksanaan Gagal NafasDocument2 pagesAlgoritma Penatalaksanaan Gagal NafasLion Sangkut Neng EndiNo ratings yet
- Initial Assessment Dan BHDDocument38 pagesInitial Assessment Dan BHDkeriatunNo ratings yet
- No. TGL Materi: Rehabilitation of Cardiovascular and Respiratory DisorderDocument6 pagesNo. TGL Materi: Rehabilitation of Cardiovascular and Respiratory DisorderFatimah AzzahraNo ratings yet
- 11 Suturing21012015Document30 pages11 Suturing21012015Putri Sari SeptirianiNo ratings yet
- Costy Panjaitan - Materi KARS SURVEILANS NEW PDFDocument40 pagesCosty Panjaitan - Materi KARS SURVEILANS NEW PDFRr.Tutik SRi HariyatiNo ratings yet
- Surveilans Health Care Associated Infections: PersiDocument49 pagesSurveilans Health Care Associated Infections: Persifebri12No ratings yet
- Terapi Cairan FullDocument34 pagesTerapi Cairan FullAnisa WahyuniartiNo ratings yet
- Final 2nd Announcement Konas Perdatin Perdici 2019 - WebsiteDocument67 pagesFinal 2nd Announcement Konas Perdatin Perdici 2019 - WebsiteWirjapratama PutraNo ratings yet
- Konsep Dasar Hais Dan Program Ppi NewDocument45 pagesKonsep Dasar Hais Dan Program Ppi NewleonardoNo ratings yet
- Calculator Dosis Obat Support Dan Vasoactive: Masukkan 55Document4 pagesCalculator Dosis Obat Support Dan Vasoactive: Masukkan 55Kaharudin KaharudinNo ratings yet
- SirkumsisiDocument24 pagesSirkumsisiBernard MarbunNo ratings yet
- Proposal Penyuluhan SenamDocument12 pagesProposal Penyuluhan SenamDechy SusmitaNo ratings yet
- Jurnal CA Paru Rifka PDFDocument8 pagesJurnal CA Paru Rifka PDFrifka riskaNo ratings yet
- HDDocument23 pagesHDSardjitoNo ratings yet
- Bu SuryaniDocument68 pagesBu SuryaniMaulana SaputraNo ratings yet
- NicardipineeeDocument8 pagesNicardipineeekevin100% (1)
- Head TraumaDocument54 pagesHead TraumaVidelia ArlitaNo ratings yet
- Jurnal Efusi PleuraDocument11 pagesJurnal Efusi PleuraAri StefanusNo ratings yet
- Soac 2021 First AnnouncementDocument13 pagesSoac 2021 First AnnouncementHendi PrihatnaNo ratings yet
- Irama JunctionalDocument18 pagesIrama JunctionalTaufik Nur YahyaNo ratings yet
- CSS Differensial Diagnosis Bayangan Radio Opaque NodulerDocument36 pagesCSS Differensial Diagnosis Bayangan Radio Opaque NodulerastiNo ratings yet
- Cavitary Lesions of Lung - S - 12 June - SSTDocument118 pagesCavitary Lesions of Lung - S - 12 June - SSTManu ChopraNo ratings yet
- Presentasi Kasus Syok HemoragikDocument75 pagesPresentasi Kasus Syok HemoragikastiNo ratings yet
- Jadwal Jaga Februari 2019Document1 pageJadwal Jaga Februari 2019astiNo ratings yet
- Jadwal Jaga Agustus 2018Document1 pageJadwal Jaga Agustus 2018astiNo ratings yet
- Learn Guide 0607Document43 pagesLearn Guide 0607astiNo ratings yet
- Whats New in GINA 2017Document12 pagesWhats New in GINA 2017Marsha Budi ClarasatiNo ratings yet
- Abdominal Wall DefectsDocument16 pagesAbdominal Wall DefectsDesta FransiscaNo ratings yet
- CSS Differensial Diagnosis Bayangan Radio Opaque NodulerDocument36 pagesCSS Differensial Diagnosis Bayangan Radio Opaque NodulerastiNo ratings yet
- HBV SerologyDocument2 pagesHBV SerologyastiNo ratings yet
- Respiratory Failure Mechanical VentilationDocument37 pagesRespiratory Failure Mechanical Ventilationawakepull312No ratings yet
- CSS Radio Opaque Nodular (Suci)Document27 pagesCSS Radio Opaque Nodular (Suci)astiNo ratings yet
- Jadwal Harian 2015Document2 pagesJadwal Harian 2015astiNo ratings yet
- COVID 19 Death Summary 11-30-2020Document1 pageCOVID 19 Death Summary 11-30-2020Live 5 NewsNo ratings yet
- ACP (American College of Physicians) Medicine-2006 PDFDocument3,054 pagesACP (American College of Physicians) Medicine-2006 PDFPuskesmasmedandenaiNo ratings yet
- Aerobic Gram-Negative BacilliDocument7 pagesAerobic Gram-Negative BacilliNhoz DoHoNo ratings yet
- Plagiarism PracticeDocument3 pagesPlagiarism PracticeingridguerreroocampoNo ratings yet
- 14.falra Rachmadiva - Xii Mipa 3 - Tugas Pertemuan 4 KD 3.6Document3 pages14.falra Rachmadiva - Xii Mipa 3 - Tugas Pertemuan 4 KD 3.6TasyaNo ratings yet
- Show Questions One by OneDocument12 pagesShow Questions One by OneCharlie Cheng-Ying HsiehNo ratings yet
- Do-It-Yourself Colloidal Silver Generator PlansDocument21 pagesDo-It-Yourself Colloidal Silver Generator Plansglvl88100% (3)
- Models of Health Promotion and Illness Prevention 1Document7 pagesModels of Health Promotion and Illness Prevention 1Krishnaveni MurugeshNo ratings yet
- Arroyo AdministrationDocument13 pagesArroyo AdministrationAngely Mae MontecalvoNo ratings yet
- Cell Salt Reference ChartDocument3 pagesCell Salt Reference ChartRidalyn Adrenalyn100% (7)
- What Are Your Opinions On This?: Fast FoodDocument4 pagesWhat Are Your Opinions On This?: Fast FoodTrân LêNo ratings yet
- Housing Light VentilationDocument34 pagesHousing Light VentilationHarshal SabaneNo ratings yet
- Using GIS in Global HealthDocument24 pagesUsing GIS in Global HealthCornelius AbbahNo ratings yet
- COVID 19 A Goldilocks ConditionDocument4 pagesCOVID 19 A Goldilocks ConditionRhollea Jane BustoNo ratings yet
- Fever With HemiplegiaDocument65 pagesFever With HemiplegiaMohit JainNo ratings yet
- Examining Joints: How To Succeed in Clinical ExaminationsDocument12 pagesExamining Joints: How To Succeed in Clinical ExaminationsimperiallightNo ratings yet
- Country Presentation MaldivesDocument11 pagesCountry Presentation MaldivesEndah PutriNo ratings yet
- Thyroid CrisisDocument20 pagesThyroid CrisisJeffrey DyerNo ratings yet
- PPE-Conducted Partnership Appreciation and Other School Based Initiatives NarrativeDocument2 pagesPPE-Conducted Partnership Appreciation and Other School Based Initiatives NarrativeCarlz BrianNo ratings yet
- Hiv/Aids: Prof. Dr. Ram Sharan Mehta Medical-Surgical Nursing DepartmentDocument196 pagesHiv/Aids: Prof. Dr. Ram Sharan Mehta Medical-Surgical Nursing DepartmentDavid Sergio Salas VargasNo ratings yet
- Russel Body - Cause of Cancer and DeathDocument12 pagesRussel Body - Cause of Cancer and DeathAndré AmorimNo ratings yet
- EpilepsyDocument38 pagesEpilepsyJareena BegumNo ratings yet
- DiverticulitaDocument6 pagesDiverticulitaoxichinolinNo ratings yet
- New Lifebuoy Soap Ad AnalysisDocument18 pagesNew Lifebuoy Soap Ad AnalysisAmit Pathak0% (1)
- Inflammatory Arthritis (SDD)Document45 pagesInflammatory Arthritis (SDD)Fera MulidarNo ratings yet
- Giardiasis Dan LeismaniaDocument39 pagesGiardiasis Dan LeismaniaSurya PradnyaNo ratings yet
- Formative M4 La1 Question 1 (1 Point) Text 1 Questions 1 - 5Document6 pagesFormative M4 La1 Question 1 (1 Point) Text 1 Questions 1 - 5teuku aditiyaNo ratings yet
- Press Release - Revised Presidential Itinerary To Lower EasternDocument2 pagesPress Release - Revised Presidential Itinerary To Lower EasternState House KenyaNo ratings yet
- Aryan Economics ActivityDocument3 pagesAryan Economics ActivityAryan AgarwalNo ratings yet
- ScabiesDocument6 pagesScabiesJayson ShieldsNo ratings yet