You might also like
- Trauma Care Manual-CRC Press Ian Greaves (Editor), Sir Keith Porter (Editor), Jeff Garner (Editor) - (2021)Document595 pagesTrauma Care Manual-CRC Press Ian Greaves (Editor), Sir Keith Porter (Editor), Jeff Garner (Editor) - (2021)Silvio danteNo ratings yet
- Time Table FCCS OB 13 - 14 Maret SbyDocument4 pagesTime Table FCCS OB 13 - 14 Maret SbyLina SusantiNo ratings yet
- Dubai Healthcare Professional Licensing Guide - Final - 2Document141 pagesDubai Healthcare Professional Licensing Guide - Final - 2Fahad IqbalNo ratings yet
- Lawton BrodyDocument1 pageLawton BrodySamuelEfraimRuntulaloNo ratings yet
- Gangguan sentral dapat disebabkan oleh:- Cedera otak/stroke- Infeksi Sistem Saraf Pusat (SSP) seperti meningitis- Hipoksia/hipoksia- Overdosis obat-obatan2. PERIFERDocument77 pagesGangguan sentral dapat disebabkan oleh:- Cedera otak/stroke- Infeksi Sistem Saraf Pusat (SSP) seperti meningitis- Hipoksia/hipoksia- Overdosis obat-obatan2. PERIFERpkm cgdmNo ratings yet
- Emergency Life Support AlgorithmDocument43 pagesEmergency Life Support AlgorithmDADASDSANo ratings yet
- ATCN 2013 Faculty Update (July 23)Document15 pagesATCN 2013 Faculty Update (July 23)Opi SaNg MadRidistas100% (1)
- Acute Coronary SyndromeDocument40 pagesAcute Coronary SyndromeJohanNo ratings yet
- ACLS TeoriDocument27 pagesACLS TeoriTita Luthfia100% (1)
- BLS in ObstetricsDocument21 pagesBLS in ObstetricsDyadina Nani100% (3)
- Acut Coronary Syndrome: Joko Sutrisno, S.Kep, NsDocument54 pagesAcut Coronary Syndrome: Joko Sutrisno, S.Kep, NsJokoSutrisnoNo ratings yet
- Kuliah EkgDocument30 pagesKuliah EkgMuhammad Ari AnugrahNo ratings yet
- Basic Life SupportDocument101 pagesBasic Life SupportMasyfuk Zuhdi JamhurNo ratings yet
- Terapi Cairan: Pembimbing: Dr. Dr. Bobby Setiadi Dharmawan, SpaDocument45 pagesTerapi Cairan: Pembimbing: Dr. Dr. Bobby Setiadi Dharmawan, SpaAdamilzaryFikryNo ratings yet
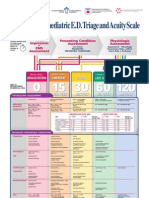
- Paediatric Triage PosterDocument1 pagePaediatric Triage PosterGenaro Olmos Garcia100% (2)
- Gawat Darurat Paru OK RevisedDocument121 pagesGawat Darurat Paru OK RevisedNasayu Nadia Santika AyuNo ratings yet
- Otsuka CairanDocument60 pagesOtsuka Cairan_LipRaa_No ratings yet
- On CPRDocument32 pagesOn CPRPiyush Dutta100% (1)
- Resusitasi Pada AnakDocument43 pagesResusitasi Pada AnakSondang Herikson PanjaitanNo ratings yet
- DefibrilasiDocument53 pagesDefibrilasiEninta Karyana MNo ratings yet
- Bantuan Hidup Dasar Dan TriageDocument30 pagesBantuan Hidup Dasar Dan TriageAtika SugiartoNo ratings yet
- Kegawatdaruratan Pada Anak Dan Bayi: Kepaniteraan Klinik Emergensi RSUP Fatmawati Jakarta FKIK UIN Syarif HidayatullahDocument81 pagesKegawatdaruratan Pada Anak Dan Bayi: Kepaniteraan Klinik Emergensi RSUP Fatmawati Jakarta FKIK UIN Syarif HidayatullahJavar SodicNo ratings yet
- AMA Specialty CodesDocument2 pagesAMA Specialty Codesamit_sethi78No ratings yet
- Gangguan Dan Keseimbangan Cairan Dan ElektrolitDocument37 pagesGangguan Dan Keseimbangan Cairan Dan ElektrolitFyana PutriNo ratings yet
- AHA Vs ERC GuidelinesDocument39 pagesAHA Vs ERC GuidelinesYoel Harianto100% (2)
- Code Blue System Di RS 2Document51 pagesCode Blue System Di RS 2Ayuningtyas Dian100% (1)
- Perfusion IndexDocument6 pagesPerfusion IndexIsmael Pérez RuizNo ratings yet
- ICU Medical Supplies InventoryDocument8 pagesICU Medical Supplies Inventoryizaura hanaNo ratings yet
- Kuliah Spine TraumaDocument91 pagesKuliah Spine Traumatutor tujuhNo ratings yet
- Bls Question 1Document7 pagesBls Question 1balderas135384No ratings yet
- 21.gigitan Ular (Snake Bite)Document16 pages21.gigitan Ular (Snake Bite)Priati Mprit100% (1)
- Resusitasi NeonatusDocument22 pagesResusitasi NeonatusnikkitaihsanNo ratings yet
- Mengenal Resusitasi Pada Anak Dan Bayi Bagi Perawat PemulaDocument15 pagesMengenal Resusitasi Pada Anak Dan Bayi Bagi Perawat PemulaSiti Krisan WijayaNo ratings yet
- Konsep EWS Di RSDocument50 pagesKonsep EWS Di RSkencaNo ratings yet
- Cardiology Workshop HighlightsDocument32 pagesCardiology Workshop HighlightsChristabella Natalia WijayaNo ratings yet
- Final Announcement Book 26th ASMIHA 2017-1Document47 pagesFinal Announcement Book 26th ASMIHA 2017-1d.ramadhanNo ratings yet
- Dianosis Dan Resusitasi Pada Pasien Syok Perdarahan &Document31 pagesDianosis Dan Resusitasi Pada Pasien Syok Perdarahan &Strata PertiwiNo ratings yet
- 2010 Integrated Updated Circulation ACLS Tachycardia AlgorithmDocument1 page2010 Integrated Updated Circulation ACLS Tachycardia AlgorithmRyggie ComelonNo ratings yet
- Extubation Criteria & Delayed EmergenceDocument3 pagesExtubation Criteria & Delayed EmergenceAnonymous OlS0WZwNo ratings yet
- Advance Cardiac Life SupportDocument18 pagesAdvance Cardiac Life Supporttepat rshsNo ratings yet
- Refreshing DHFDocument13 pagesRefreshing DHFNia Nurhayati ZakiahNo ratings yet
- Materi PelatihanDocument1 pageMateri PelatihanEric PhangestuNo ratings yet
- ICD 10 - ParuDocument3 pagesICD 10 - ParuAlexanderKam100% (1)
- Prof - Dr. Ruswan Dachlan, SP An KIC Dept - of Anaesthesiology & Intensive Care FKUIDocument71 pagesProf - Dr. Ruswan Dachlan, SP An KIC Dept - of Anaesthesiology & Intensive Care FKUIFerdy ErawanNo ratings yet
- Syok HipovolemikDocument40 pagesSyok HipovolemikIrma Purnama Purnama100% (1)
- Saran Hasil Mcu InggrisDocument3 pagesSaran Hasil Mcu Inggrisapril babyNo ratings yet
- Kriteria Intubasi Dan EkstubasiDocument31 pagesKriteria Intubasi Dan Ekstubasifml grNo ratings yet
- Diagnosis dan Tatalaksana Awal Stroke dan SAH di IGDDocument26 pagesDiagnosis dan Tatalaksana Awal Stroke dan SAH di IGDekaNo ratings yet
- K-5 Pathophysiology of Cyanotic Congenital Heart DefectsDocument15 pagesK-5 Pathophysiology of Cyanotic Congenital Heart DefectsJessica GintingNo ratings yet
- Integrated Emergency and Disaster Management System in DIYDocument49 pagesIntegrated Emergency and Disaster Management System in DIYHari Mas KuncoroNo ratings yet
- Sop Journal ReadingDocument6 pagesSop Journal Readingriki_rdnNo ratings yet
- First Year 2019docxDocument262 pagesFirst Year 2019docxCherry100% (1)
- Soac 2021 First AnnouncementDocument13 pagesSoac 2021 First AnnouncementHendi PrihatnaNo ratings yet
- ATLS FatmawatiDocument35 pagesATLS FatmawatiAnindya Anjas PutriaviNo ratings yet
- Prehospital Emergency Cardiac Care for STEMI PatientsDocument100 pagesPrehospital Emergency Cardiac Care for STEMI PatientstammypusphitarNo ratings yet
- Code Blue Response at Jasa Kartini HospitalDocument16 pagesCode Blue Response at Jasa Kartini Hospitalannisamuti10No ratings yet
- Terapi Cairan Pada Pasien Shock HemooragikDocument41 pagesTerapi Cairan Pada Pasien Shock HemooragikNur Syifa FadhilahNo ratings yet
- EKG Interpretasi Dan Lethal Aritmia: Aan NuraeniDocument34 pagesEKG Interpretasi Dan Lethal Aritmia: Aan NuraeniCitra Marchelina Novilini100% (1)
- Anestesi Residen DaftarDocument12 pagesAnestesi Residen DaftarfikhryNo ratings yet
- Dosis Obat Igd PDFDocument3 pagesDosis Obat Igd PDFRiyadila FajarizaNo ratings yet
- Announcement IndoanesthesiaDocument24 pagesAnnouncement IndoanesthesiaAndrian100% (1)
- Dr. Hasyim Kasim, HipertensiDocument50 pagesDr. Hasyim Kasim, HipertensiImaji Corp MakassarNo ratings yet
- Askep MCI - AchirmanDocument53 pagesAskep MCI - AchirmanmarthaNo ratings yet
- Head circumference growth chart for baby girlsDocument1 pageHead circumference growth chart for baby girlsNia Tri Mulyani100% (1)
- Materi DR Rita Zahara NewDocument31 pagesMateri DR Rita Zahara NewIrfanNo ratings yet
- Daftar Nutrisi ParenteralDocument6 pagesDaftar Nutrisi Parenteralcitrahdyn100% (1)
- Case Discussion on Mrs. K's HospitalizationDocument40 pagesCase Discussion on Mrs. K's HospitalizationHiLmanNo ratings yet
- Understanding Tachycardia and Bradycardia ClassificationsDocument18 pagesUnderstanding Tachycardia and Bradycardia ClassificationsZega AgustianNo ratings yet
- Jumlah Tetesan Infus MakroDocument2 pagesJumlah Tetesan Infus MakroMamanya Ef Taya ThalitaNo ratings yet
- Cardiopulmonary ResuscitationDocument69 pagesCardiopulmonary ResuscitationSamuel Ojonugwa AuduNo ratings yet
- Cardiac ArrestDocument19 pagesCardiac ArrestJohanNo ratings yet
- 4 - Guidelines Pneumothorax BTSDocument15 pages4 - Guidelines Pneumothorax BTSNyoman YudiartonoNo ratings yet
- Instrumental Activities of Daily LivingDocument1 pageInstrumental Activities of Daily LivingJohanNo ratings yet
- ABC of BurnsDocument37 pagesABC of Burnsiraklisd100% (2)
- ACG Guideline AcutePancreatitis September 2013Document16 pagesACG Guideline AcutePancreatitis September 2013gorditomaloNo ratings yet
- Adl TableDocument3 pagesAdl TableNadia IndriNo ratings yet
- Airway ManagementDocument50 pagesAirway ManagementJohanNo ratings yet
- BreathingDocument14 pagesBreathingJohanNo ratings yet
- FESS ComplicationsDocument17 pagesFESS ComplicationsJohanNo ratings yet
- SinusDocument49 pagesSinusmomocamuiNo ratings yet
- SODocument9 pagesSOJohanNo ratings yet
- Liver Transplantation: HCV Disease ProgressionDocument6 pagesLiver Transplantation: HCV Disease ProgressionJohanNo ratings yet
- Qsi 3081 - Ikhtisas Hoki: Critique Journal ArticleDocument3 pagesQsi 3081 - Ikhtisas Hoki: Critique Journal ArticlenurayunirahimNo ratings yet
- 2nd Quarter PEDocument49 pages2nd Quarter PEhunterstrike61No ratings yet
- There Is A Common Acronym in BLS Used To Guide Providers in The Appropriate Steps To Assess and Treat Patients in Respiratory and Cardiac DistressDocument3 pagesThere Is A Common Acronym in BLS Used To Guide Providers in The Appropriate Steps To Assess and Treat Patients in Respiratory and Cardiac DistressMc SuanNo ratings yet
- Mechanical Ventilation Modes and TypesDocument40 pagesMechanical Ventilation Modes and TypesAmol TemkarNo ratings yet
- Impact of online appointment systems on healthcare access and costsDocument9 pagesImpact of online appointment systems on healthcare access and costspatricia gunioNo ratings yet
- Out of Hospital Spinal Immobilization - Its Effect On Neurologic InjuryDocument7 pagesOut of Hospital Spinal Immobilization - Its Effect On Neurologic InjuryJade OttoniNo ratings yet
- First Aid: 15 Minutes Presentation at Ald Ersgate CollegeDocument19 pagesFirst Aid: 15 Minutes Presentation at Ald Ersgate CollegeEmmanuel John Dela CruzNo ratings yet
- Pals 2020 Nuevas ConsideracionesDocument1 pagePals 2020 Nuevas Consideracionesfrancia perezNo ratings yet
- Governing disasters challenges to integrated emergency networksDocument6 pagesGoverning disasters challenges to integrated emergency networksrobertNo ratings yet
- 1503971634VIVO Basic Emergency Medical Technician (EMT B) 2 M PDFDocument1 page1503971634VIVO Basic Emergency Medical Technician (EMT B) 2 M PDFRiya SachanNo ratings yet
- Underreporting of Traumatic Brain Injuries in Pediatric Craniomaxillofacial Trauma - A 20-Year Retrospective Cohort StudyDocument10 pagesUnderreporting of Traumatic Brain Injuries in Pediatric Craniomaxillofacial Trauma - A 20-Year Retrospective Cohort StudySebastiano Sega100% (1)
- Emergency Medical Services Unit Patient AssessmentDocument4 pagesEmergency Medical Services Unit Patient Assessmentariel sanchezNo ratings yet
- Surat Panggilan Ke 2Document8 pagesSurat Panggilan Ke 2AlyssaCamiliaNo ratings yet
- Basic Life Support ChecklistDocument1 pageBasic Life Support ChecklistJoshua DauzNo ratings yet
- BLSPPT 180126100212 PDFDocument58 pagesBLSPPT 180126100212 PDFAdolfo Sven Gomez MolinaNo ratings yet
- Cert Imp234y2x4sfDocument1 pageCert Imp234y2x4sfapi-653788186No ratings yet
- ICU Infection Sources in Sepsis PatientsDocument5 pagesICU Infection Sources in Sepsis PatientsEndah Novianti SoenarsinNo ratings yet
- A Comprehensive Look at Caritas Health Associates' Marketing Professional ProgramDocument240 pagesA Comprehensive Look at Caritas Health Associates' Marketing Professional ProgramMarcu QuerubinNo ratings yet
- 3 Abdominal TraumaDocument31 pages3 Abdominal Traumadoc-fahad aftabNo ratings yet
- EMS Field Handbook (Revision 1) PDFDocument61 pagesEMS Field Handbook (Revision 1) PDFAnonymous qAEhQo1No ratings yet
- HematothoraxDocument15 pagesHematothoraxmail junkNo ratings yet
- Cardiac ArrestDocument21 pagesCardiac Arrestashrf seadNo ratings yet