You might also like
- Proposed Ordinance Brgy. Health Board Salamanca PDFDocument4 pagesProposed Ordinance Brgy. Health Board Salamanca PDFalfredtan6288No ratings yet
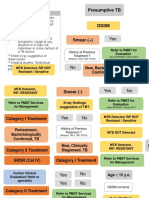
- Flowchart TB DOTSDocument11 pagesFlowchart TB DOTSalfredtan6288No ratings yet
- Informative Speech OutlineDocument3 pagesInformative Speech Outlineapi-250554127100% (1)
- Consumer E-Health ProgramDocument10 pagesConsumer E-Health ProgramONC for Health Information Technology100% (1)
- NANDA Nursing Diagnosis Domain 1Document8 pagesNANDA Nursing Diagnosis Domain 1krystaliciousNo ratings yet
- ILEP Stigma GuidelinesDocument48 pagesILEP Stigma GuidelinesPeter Indra SeptianNo ratings yet
- Qualitative Research MethodologyDocument36 pagesQualitative Research Methodologygrootpyp67% (3)
- StepsDocument4 pagesStepsshrikantNo ratings yet
- Research Definitions, Types, Problems and ObjectivesDocument66 pagesResearch Definitions, Types, Problems and ObjectivesSolomon MeseretNo ratings yet
- Evidence Based Practice ProcessDocument29 pagesEvidence Based Practice ProcessDrmirfat AlkashifNo ratings yet
- DJ HospitalDocument30 pagesDJ Hospitaldineshjaiswal1212No ratings yet
- Query Health - Rich Elmore - HIT Policy Committee 2011-09-14Document20 pagesQuery Health - Rich Elmore - HIT Policy Committee 2011-09-14Rich ElmoreNo ratings yet
- Critical Appraisal Trial (Cat) : Z0Bia Naseem LecturerDocument30 pagesCritical Appraisal Trial (Cat) : Z0Bia Naseem LecturerAiqa QaziNo ratings yet
- Tool To Estimate Patients' CostsDocument83 pagesTool To Estimate Patients' CostsAgus FitrianggaNo ratings yet
- Brief 8 Quasi-Experimental Design EngDocument16 pagesBrief 8 Quasi-Experimental Design Engpresi_studentNo ratings yet
- Running Head: Effectiveness of Dementia Inteventions 1Document12 pagesRunning Head: Effectiveness of Dementia Inteventions 1John Mureithi NjugunaNo ratings yet
- Research MethodologyDocument24 pagesResearch MethodologyHendri Johan Tambunan11No ratings yet
- The KAP Survey ModelDocument38 pagesThe KAP Survey ModelRainer Danny Poluan Mamahit100% (4)
- Module I - Group WorkDocument6 pagesModule I - Group WorkNur SanaaniNo ratings yet
- How To Explore The Needs of Informal Caregivers of Individuals With Cognitive Impairment in Alzheimer's Disease or Related DiseasesDocument18 pagesHow To Explore The Needs of Informal Caregivers of Individuals With Cognitive Impairment in Alzheimer's Disease or Related DiseasesCristina MPNo ratings yet
- The Common Threads in ProgramDocument5 pagesThe Common Threads in Programdate6No ratings yet
- A Guiding Using Qualitative Research MethodsDocument37 pagesA Guiding Using Qualitative Research Methodsd_anto781063100% (1)
- Critical Appraisal of Cohort Studies EBMP 1000e108Document2 pagesCritical Appraisal of Cohort Studies EBMP 1000e108thetaggerung100% (1)
- Theories and Models in AIDS PREVENTIONDocument14 pagesTheories and Models in AIDS PREVENTIONMatin Ahmad KhanNo ratings yet
- Literature Review Publication BiasDocument4 pagesLiterature Review Publication Biasc5qx9hq5100% (1)
- Research in Health Care: How To Learn Mixed Methods ResearchDocument6 pagesResearch in Health Care: How To Learn Mixed Methods ResearchMuhammad PanjiNo ratings yet
- Focus Group Discussions - A Step-By-Step Guide: University of Limpopo & VLIR Project South AfricaDocument83 pagesFocus Group Discussions - A Step-By-Step Guide: University of Limpopo & VLIR Project South AfricaSaiful Islam ShawonNo ratings yet
- Running Head: Effectiveness of Dementia Inteventions 1Document17 pagesRunning Head: Effectiveness of Dementia Inteventions 1John Mureithi NjugunaNo ratings yet
- Communication 2Document30 pagesCommunication 2ماجد الثبيتيNo ratings yet
- ANP - EBP Model ASHDocument12 pagesANP - EBP Model ASHManoj BalaNo ratings yet
- Evidence Based Practice in NursingDocument9 pagesEvidence Based Practice in NursingSimran Chauhan100% (2)
- Proposal Writing: Dr. S. Sharaf Ali ShahDocument33 pagesProposal Writing: Dr. S. Sharaf Ali Shahmama the mirNo ratings yet
- Week 4 Midterm Study GuideDocument7 pagesWeek 4 Midterm Study GuideDeanne VerschureNo ratings yet
- Fall Prevention Research PaperDocument8 pagesFall Prevention Research Paperorlfgcvkg100% (1)
- Effective Strategies For Scaling Up Evidence-Based PDFDocument13 pagesEffective Strategies For Scaling Up Evidence-Based PDFAbraham LebezaNo ratings yet
- KN ClinicalGuidelines2Document2 pagesKN ClinicalGuidelines2Mhmd IrakyNo ratings yet
- Reporting Guidelines For Implementation and Operational ResearchDocument7 pagesReporting Guidelines For Implementation and Operational ResearchDanNo ratings yet
- Attitudes of Health Professionals To The Development of Information Systems and The Use of InformationDocument39 pagesAttitudes of Health Professionals To The Development of Information Systems and The Use of InformationMeer TanveerNo ratings yet
- Guidebook Evaluation Stigma Patrick CarriganDocument66 pagesGuidebook Evaluation Stigma Patrick CarriganJana ChihaiNo ratings yet
- Piloting A New Approach in Primary Care To Identify, Assess and Support Carers of People With Terminal Illnesses: A Feasibility StudyDocument9 pagesPiloting A New Approach in Primary Care To Identify, Assess and Support Carers of People With Terminal Illnesses: A Feasibility StudyCarolina UrrutiaNo ratings yet
- PepsicolaHPAguidancedocument PDFDocument4 pagesPepsicolaHPAguidancedocument PDFAnonymous qemC1CybLNo ratings yet
- Roemenie Evidence Based Practice ExercisesDocument2 pagesRoemenie Evidence Based Practice ExercisesCristinaSohorcaNo ratings yet
- Putoolssect7 PDFDocument63 pagesPutoolssect7 PDFRinaNo ratings yet
- Needs Assessment CycleDocument8 pagesNeeds Assessment Cycleapi-273554555No ratings yet
- Prevention and Health Promotion 2023SSDocument39 pagesPrevention and Health Promotion 2023SSzeynepNo ratings yet
- محاضرة رقم 3 البرهانDocument38 pagesمحاضرة رقم 3 البرهانareejjooryNo ratings yet
- Nursing ProcessDocument14 pagesNursing Processrubycorazon_ediza100% (1)
- HESM 375 Mid Term Study NotesDocument4 pagesHESM 375 Mid Term Study NotesJenny PriorNo ratings yet
- Simulated Clinic Tips and PitfallsDocument27 pagesSimulated Clinic Tips and PitfallsFayzaRayesNo ratings yet
- CalderMM Rounds Guide 2012Document17 pagesCalderMM Rounds Guide 2012Fate ChanNo ratings yet
- Guideline Kap Jan Mar04Document3 pagesGuideline Kap Jan Mar04Sidik Syah PutraNo ratings yet
- Understanding The Public Health and Private Medical Care SystemDocument56 pagesUnderstanding The Public Health and Private Medical Care Systemriski novitaNo ratings yet
- Randomised Controlled Trials - Gold Standard or Fool's Gold? The Role of Experimental Methods in Voluntary Sector Impact Assessment (Cupitt 2015)Document9 pagesRandomised Controlled Trials - Gold Standard or Fool's Gold? The Role of Experimental Methods in Voluntary Sector Impact Assessment (Cupitt 2015)NCVONo ratings yet
- CPHQ PrepDocument50 pagesCPHQ PrepTOBIN6319_39572798689% (9)
- Needs Assessment: What Is It?Document5 pagesNeeds Assessment: What Is It?Fidias FernandezNo ratings yet
- Outcome Research Methodology: BY Sumaira Naz BSN, MPHDocument40 pagesOutcome Research Methodology: BY Sumaira Naz BSN, MPHFatima AnxariNo ratings yet
- Design ThinkingDocument29 pagesDesign Thinkingsinghsaurabhh91No ratings yet
- Curso de Buena Practica Clínica y Ética e Investigación ConductualDocument10 pagesCurso de Buena Practica Clínica y Ética e Investigación ConductualHalberto GilNo ratings yet
- Introduction To Clinical Decision MakingDocument40 pagesIntroduction To Clinical Decision MakingVANSHIKANo ratings yet
- PleasantDocument31 pagesPleasantDavid ResnickNo ratings yet
- NUR 816: Week1 NotesDocument21 pagesNUR 816: Week1 NotesAlvia MagnoNo ratings yet
- Using Mixed Methods Approach To Enhance and Validate Your ResearchDocument82 pagesUsing Mixed Methods Approach To Enhance and Validate Your ResearchVickneswary BathumalaiNo ratings yet
- HelminthsDocument15 pagesHelminthsalfredtan6288No ratings yet
- Ma. Michelle P. Acosta, RN, MN: Senior Health Program OfficerDocument15 pagesMa. Michelle P. Acosta, RN, MN: Senior Health Program Officeralfredtan6288No ratings yet
- FP Misconceptions and BehaviorsDocument6 pagesFP Misconceptions and Behaviorsalfredtan6288No ratings yet
- NRPCPDocument28 pagesNRPCPalfredtan6288No ratings yet
- Recording Form 1 Pneumococal Vaccine MasterlistDocument1 pageRecording Form 1 Pneumococal Vaccine Masterlistalfredtan6288No ratings yet
- Err:514 Err:514: Non-Communicable Disease CalculatorDocument2 pagesErr:514 Err:514: Non-Communicable Disease Calculatoralfredtan6288No ratings yet
- Form 2a NTP Referral Form v2003Document2 pagesForm 2a NTP Referral Form v2003alfredtan6288100% (1)
- Session 1b - Barriers To An Effective TB ControlDocument5 pagesSession 1b - Barriers To An Effective TB Controlalfredtan6288No ratings yet
- Session 1b - Barriers To An Effective TB ControlDocument5 pagesSession 1b - Barriers To An Effective TB Controlalfredtan6288No ratings yet
- Cupuncture: Victor S. SierpinaDocument6 pagesCupuncture: Victor S. SierpinaSgantzos MarkosNo ratings yet
- The Factories Act 1948Document96 pagesThe Factories Act 1948NIKITHAA ASHWINNo ratings yet
- Phobias - See What Makes Some People AfraidDocument2 pagesPhobias - See What Makes Some People Afraidbeep777No ratings yet
- UL WP Final Using Leading and Lagging Safety Indicators To Manage Workplace Health and Safety Risk V7 LR1Document10 pagesUL WP Final Using Leading and Lagging Safety Indicators To Manage Workplace Health and Safety Risk V7 LR1Nhut NguyenNo ratings yet
- Interview Paper SW 3010Document7 pagesInterview Paper SW 3010api-319252753No ratings yet
- History of Toxicity TestingDocument4 pagesHistory of Toxicity TestingIja Nur100% (1)
- Assignment No 1 bt502 SeminarDocument15 pagesAssignment No 1 bt502 SeminarMashal WakeelaNo ratings yet
- Managerial Epidemiology Concepts and Case, 2d Ed.: Full TextDocument2 pagesManagerial Epidemiology Concepts and Case, 2d Ed.: Full TextlovesunsetNo ratings yet
- Pengaruh Penambahan Kayu Manis TerhadapDocument8 pagesPengaruh Penambahan Kayu Manis TerhadapIbnu SetyawanNo ratings yet
- You Exec - Coronavirus Management Kit FreeDocument25 pagesYou Exec - Coronavirus Management Kit FreeNidaNo ratings yet
- 3390 3396 PDFDocument7 pages3390 3396 PDFXavier Alexandro Ríos SalinasNo ratings yet
- Introduction of Air Ambulance Services in IndiaDocument5 pagesIntroduction of Air Ambulance Services in Indiaprithvinatarajan100% (1)
- Chapter 2Document15 pagesChapter 2Daniel John LingamenNo ratings yet
- Normal Random Blood Sugar - Google SearchDocument1 pageNormal Random Blood Sugar - Google SearchmechNo ratings yet
- A Filipino Worker's Resilience Amidst Covid-19 PandemicDocument15 pagesA Filipino Worker's Resilience Amidst Covid-19 PandemicVin Nicole Salazar Revilla67% (3)
- BibliographyDocument2 pagesBibliographyelvie21No ratings yet
- Temy Dlya Napisania Esse V EGE Po Angliyskomu YazykuDocument7 pagesTemy Dlya Napisania Esse V EGE Po Angliyskomu YazykuElena StepanovaNo ratings yet
- Module 7 Lesson 4Document31 pagesModule 7 Lesson 4MA EDYLYN NOGUERRANo ratings yet
- Accredited Social Health Activist: Ms - Neethu Vincent Asst Professor KVM College of NursingDocument18 pagesAccredited Social Health Activist: Ms - Neethu Vincent Asst Professor KVM College of NursingNeethu VincentNo ratings yet
- Application of The MASCC and CISNE Risk-Strati Fication Scores To Identify Low-Risk Febrile Neutropenic Patients in The Emergency DepartmentDocument10 pagesApplication of The MASCC and CISNE Risk-Strati Fication Scores To Identify Low-Risk Febrile Neutropenic Patients in The Emergency DepartmentwiraNo ratings yet
- Format Nutritional StatusDocument43 pagesFormat Nutritional StatusDirkie Meteoro Rufin83% (6)
- MScHandbook Imperial Chemical EnggDocument87 pagesMScHandbook Imperial Chemical EnggMurugeshNo ratings yet
- San Antonio and Bexar County Petition For TRO Against Gov. Abbott Over Local Control of COVID-19 Prevention EffortsDocument29 pagesSan Antonio and Bexar County Petition For TRO Against Gov. Abbott Over Local Control of COVID-19 Prevention EffortsKENS 5No ratings yet
- Hili MallDocument7 pagesHili Mallvenkatesh snkNo ratings yet
- BrainHealthAssessment ReportDocument14 pagesBrainHealthAssessment ReportJoe CohenNo ratings yet
- The Effects of Sleep Deprivation On Your BodyDocument21 pagesThe Effects of Sleep Deprivation On Your BodyFaradilah Binti Ajma'inNo ratings yet
- Bioethics EssayDocument7 pagesBioethics Essayapi-336568283No ratings yet