You might also like
- Hyponatremia (Emphasis On SIADH) : DR Adeyemo A. ODocument57 pagesHyponatremia (Emphasis On SIADH) : DR Adeyemo A. OAdeyemo AyoadeNo ratings yet
- Neuroimaging and DNA Profiling New AvenuesDocument52 pagesNeuroimaging and DNA Profiling New AvenuesDr-Ajay TripathiNo ratings yet
- HyponatraemiaDocument16 pagesHyponatraemiaRaluca LeucaNo ratings yet
- HyponatremiaDocument6 pagesHyponatremiaJaymart Saclolo CostillasNo ratings yet
- Hyponatremia: BY: Dr. Sammon K TareenDocument35 pagesHyponatremia: BY: Dr. Sammon K TareenSammon TareenNo ratings yet
- The Hyponatremic Patient: A Systematic Approach To Laboratory DiagnosisDocument7 pagesThe Hyponatremic Patient: A Systematic Approach To Laboratory DiagnosisJuen LohNo ratings yet
- HyponatremiaDocument20 pagesHyponatremiamanjaruNo ratings yet
- Diabetes Insipidus & Syndrome of Inappropiate Antidiuretic HormoneDocument16 pagesDiabetes Insipidus & Syndrome of Inappropiate Antidiuretic HormoneStephanie RiveraNo ratings yet
- Final Version of PropagandaDocument41 pagesFinal Version of PropagandaZara IftikharNo ratings yet
- Electrolyte DisordersDocument10 pagesElectrolyte DisordersSlavicaNo ratings yet
- Hyponatremia and HypernatremiaDocument39 pagesHyponatremia and HypernatremiaManhal A AbdulkaderNo ratings yet
- How I Approach Hyponatraemia: CME EndocrinologyDocument6 pagesHow I Approach Hyponatraemia: CME EndocrinologyFernando Re TaNo ratings yet
- SIADH (Syndrome of Inapproperiate Antidiuretic Hormone Secretion)Document11 pagesSIADH (Syndrome of Inapproperiate Antidiuretic Hormone Secretion)itsmesubu100% (2)
- Fluid & Electrolyte Management & Acid Base Disorders: Alice Augustin Amina S Anagha P RDocument47 pagesFluid & Electrolyte Management & Acid Base Disorders: Alice Augustin Amina S Anagha P RAsif AbbasNo ratings yet
- A Systematic Approach To The Hyponatremic Patient: Iva Ratkoviê-Gusiê, Petar Kes And Vanja Baπiê-KesDocument10 pagesA Systematic Approach To The Hyponatremic Patient: Iva Ratkoviê-Gusiê, Petar Kes And Vanja Baπiê-KesTio Prima SNo ratings yet
- Plications of HemodialysisDocument30 pagesPlications of HemodialysisAISHWARYA T DNo ratings yet
- Diabetes Insipidus, Siadh and Cerebral Salt-WastingDocument33 pagesDiabetes Insipidus, Siadh and Cerebral Salt-WastingEuphrasiaNo ratings yet
- Hypokalaemia and HyperkalaemiaDocument39 pagesHypokalaemia and HyperkalaemiaRZ NgNo ratings yet
- Concept Map - HyponatremiaDocument9 pagesConcept Map - HyponatremiaElleNo ratings yet
- HiponatremiaDocument8 pagesHiponatremiaMeidistya Ayu MardhianiNo ratings yet
- M5 - Electrolyte AbnormalitiesDocument44 pagesM5 - Electrolyte AbnormalitiesVishal KumarNo ratings yet
- Pathophysiology and Etiology of The Syndrome of Inappropriate Antidiuretic Hormone Secretion (Siadh)Document24 pagesPathophysiology and Etiology of The Syndrome of Inappropriate Antidiuretic Hormone Secretion (Siadh)Urgencias E.S.E Coromoro - Centro salud CinceladaNo ratings yet
- Guidelines For The Management of HyponatraemiaDocument8 pagesGuidelines For The Management of HyponatraemiaMuhammad Amiro RasheeqNo ratings yet
- Approach To Fluid and Electrolyte Disorders and Acid-Base ProblemsDocument19 pagesApproach To Fluid and Electrolyte Disorders and Acid-Base ProblemsHigh EducationNo ratings yet
- Manajemen Anestesi Pada Uremic SyndromeDocument27 pagesManajemen Anestesi Pada Uremic SyndromeAdi Nugroho MelyanaNo ratings yet
- Fluid and Electrolytes Assignment 1. What Are The Different Processes of Body Fluid and Solutes Movement? and Give at Least 2 Examples EachDocument8 pagesFluid and Electrolytes Assignment 1. What Are The Different Processes of Body Fluid and Solutes Movement? and Give at Least 2 Examples EachAngelicaNo ratings yet
- Fluid and Electrolytes Assignment 1. What Are The Different Processes of Body Fluid and Solutes Movement? and Give at Least 2 Examples EachDocument8 pagesFluid and Electrolytes Assignment 1. What Are The Different Processes of Body Fluid and Solutes Movement? and Give at Least 2 Examples EachAngelicaNo ratings yet
- NCM 3114 Electrolyte Imbalance-2Document21 pagesNCM 3114 Electrolyte Imbalance-2Nicole Sherry M. CHEENo ratings yet
- Electrolyte Imbalances and Their Management.: by Nabawanda Saluwa Facilitator: DR - Ssebuliba MosesDocument44 pagesElectrolyte Imbalances and Their Management.: by Nabawanda Saluwa Facilitator: DR - Ssebuliba MosesNinaNo ratings yet
- Hyponatremia: Q: Discuss Hyponatremia in Clinical PracticeDocument7 pagesHyponatremia: Q: Discuss Hyponatremia in Clinical PracticemyqueenleoNo ratings yet
- Surgery YbDocument67 pagesSurgery YbTamirat geletaNo ratings yet
- Guideline, Management of HypernatremiaDocument9 pagesGuideline, Management of HypernatremiaLia Safitri Leloly100% (1)
- By DR Madhusudan C Associate Professor Department of MedicineDocument39 pagesBy DR Madhusudan C Associate Professor Department of MedicineTeena ChandranNo ratings yet
- ENDO... ElectrolyteDocument44 pagesENDO... ElectrolyteOmar AbdillahiNo ratings yet
- Chapter 16: Disorders of Serum Sodium Concentration in The Elderly PatientDocument6 pagesChapter 16: Disorders of Serum Sodium Concentration in The Elderly PatientYantimuliawatiNo ratings yet
- Fluid Deficit RevisedDocument6 pagesFluid Deficit RevisedShaira SariaNo ratings yet
- Causes of Hyponatremia in AdultsDocument18 pagesCauses of Hyponatremia in AdultsAndro Franco Florio CatalánNo ratings yet
- AldosteronismDocument48 pagesAldosteronismMiguel Cuevas DolotNo ratings yet
- HyponatremiaDocument21 pagesHyponatremiaselma100% (1)
- Chronic Kidney DiseaseDocument6 pagesChronic Kidney Diseaseashi leginNo ratings yet
- Lab Data InterpretationDocument38 pagesLab Data Interpretationraziajaffery14No ratings yet
- Fluids and Electrolytes and Acid Base PhysiologyDocument64 pagesFluids and Electrolytes and Acid Base PhysiologyJesserene Mangulad SorianoNo ratings yet
- RANASINGHE Fluid Electrolyte and Acid Base PhysiologyDocument45 pagesRANASINGHE Fluid Electrolyte and Acid Base PhysiologyDagimNo ratings yet
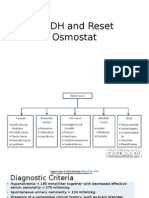
- SIADH and Reset OsmostatDocument7 pagesSIADH and Reset Osmostatsaleema11No ratings yet
- Page 1 of 6Document6 pagesPage 1 of 6Karissa MagaruNo ratings yet
- Group 1 SiadhDocument22 pagesGroup 1 SiadhFuzna DahliaNo ratings yet
- MINI ReviewDocument10 pagesMINI ReviewShamila KaruthuNo ratings yet
- Disorders of Carbohydrate Metabolism.: Abdelmoniem Saeed Mohammed Er SpecialistDocument49 pagesDisorders of Carbohydrate Metabolism.: Abdelmoniem Saeed Mohammed Er SpecialistYousef Al-AmeenNo ratings yet
- Defining SIADHDocument2 pagesDefining SIADHJohan El-Hakim Siregar100% (1)
- Indications of Dialysis in Acute Renal Failure (ARF)Document3 pagesIndications of Dialysis in Acute Renal Failure (ARF)Tariku GelesheNo ratings yet
- Hyponatremia by Vikas ParekhDocument2 pagesHyponatremia by Vikas ParekhAlimu SowNo ratings yet
- Fispatologjia e CreegullimeveDocument16 pagesFispatologjia e CreegullimeveArmar MendoNo ratings yet
- Electrolyte Imbalance: Sodium: Submitted By: Milosantos, John Francis D. Tuibeo, Ma. Arlyn P. Yu, Aldrin Anthony LDocument6 pagesElectrolyte Imbalance: Sodium: Submitted By: Milosantos, John Francis D. Tuibeo, Ma. Arlyn P. Yu, Aldrin Anthony Lnospekiko21No ratings yet
- Hyponatremia ADocument44 pagesHyponatremia ASteven Godelman100% (3)
- Acute Renal Failure Nursing Care PlanDocument15 pagesAcute Renal Failure Nursing Care PlanRanusha AnushaNo ratings yet
- 12-1 Diabetic Emergencies-HHS PDFDocument12 pages12-1 Diabetic Emergencies-HHS PDFOana DumitruNo ratings yet
- Group 1 SiadhDocument20 pagesGroup 1 SiadhArul MNo ratings yet
- Fluids Electrolytes Group 1 CompilationDocument41 pagesFluids Electrolytes Group 1 CompilationShaira SariaNo ratings yet
- Siadh & Hyponatremia: Dr. Kushal Markanday MDDocument67 pagesSiadh & Hyponatremia: Dr. Kushal Markanday MD966342100% (1)
- Identify Vein, Artery, Disc, Optic Cup, FoveaDocument30 pagesIdentify Vein, Artery, Disc, Optic Cup, FoveaAhmed AbdelgelilNo ratings yet
- Acute Confusional State ManagementDocument18 pagesAcute Confusional State ManagementAhmed AbdelgelilNo ratings yet
- CC History Mnemonics Physicals Notes/ Challenges Counsel DD WorkupDocument41 pagesCC History Mnemonics Physicals Notes/ Challenges Counsel DD WorkupAhmed AbdelgelilNo ratings yet
- 4 Tips For Passing PACES: PreparationDocument10 pages4 Tips For Passing PACES: PreparationAhmed AbdelgelilNo ratings yet
- IMPO Info For PACES (DR Shiny Moon)Document3 pagesIMPO Info For PACES (DR Shiny Moon)Ahmed AbdelgelilNo ratings yet
- My Masterclass Exam #59765: About Products Buy Institutions Exam Demo Video Demo Contact Us FAQ My Account LogoutDocument59 pagesMy Masterclass Exam #59765: About Products Buy Institutions Exam Demo Video Demo Contact Us FAQ My Account LogoutAhmed AbdelgelilNo ratings yet
- GIT MnemonicsDocument20 pagesGIT MnemonicsAhmed AbdelgelilNo ratings yet
- Doctor in Come by Service Types ReportDocument1 pageDoctor in Come by Service Types ReportAhmed AbdelgelilNo ratings yet
- My Masterclass Exam #58292: About Products Buy Institutions Exam Demo Video Demo Contact Us FAQ My Account LogoutDocument59 pagesMy Masterclass Exam #58292: About Products Buy Institutions Exam Demo Video Demo Contact Us FAQ My Account LogoutAhmed AbdelgelilNo ratings yet
- Self Assessment Sba .Philip BakerDocument196 pagesSelf Assessment Sba .Philip BakerAhmed Abdelgelil100% (2)
- Self Assessment Sba .Philip BakerDocument196 pagesSelf Assessment Sba .Philip BakerAhmed Abdelgelil100% (2)
- Paraneoplastic Syndromes Associated With LaryngealDocument15 pagesParaneoplastic Syndromes Associated With Laryngealandre halimNo ratings yet
- Ure NaDocument2 pagesUre NaKenaz Duane Peter SegayaNo ratings yet
- Endocrine System BulletsDocument28 pagesEndocrine System Bulletswinner gift flowersNo ratings yet
- Fluid and Electrolyte ImbalancesDocument57 pagesFluid and Electrolyte ImbalancesTerry Mae Atilazal SarciaNo ratings yet
- Med Surg Chap QuestionsDocument9 pagesMed Surg Chap Questionslani0% (1)
- Toronto Notes Nephrology 2015 8Document1 pageToronto Notes Nephrology 2015 8JUSASBNo ratings yet
- Critical Care Notes Clinical Pocket Guide - (Hematology Oncology)Document17 pagesCritical Care Notes Clinical Pocket Guide - (Hematology Oncology)Britanny NelsonNo ratings yet
- Canadian-Exam-Answers-2007 من امتحانات الجامعةDocument189 pagesCanadian-Exam-Answers-2007 من امتحانات الجامعةAli Toma HmedatNo ratings yet
- SNQ ExamDocument32 pagesSNQ ExamhelamahjoubmounirdmoNo ratings yet
- Internal Medicine Highlights by Conrad Fischer (2008)Document34 pagesInternal Medicine Highlights by Conrad Fischer (2008)Li Sac67% (3)
- NUR265 Exam 2 Holmes Mock Answered PDFDocument13 pagesNUR265 Exam 2 Holmes Mock Answered PDFNoemi GabayNo ratings yet
- Water An Electrolyte Metabolism and Their DisordersDocument60 pagesWater An Electrolyte Metabolism and Their DisordersAbigail AdegbuluNo ratings yet
- Electrolytes: George A. HarwellDocument29 pagesElectrolytes: George A. HarwellWho Knows100% (1)
- SIADH, DI and Cerebral Salt Wasting: Karim Rafaat, MDDocument54 pagesSIADH, DI and Cerebral Salt Wasting: Karim Rafaat, MDMahendra PrasetyoNo ratings yet
- Dokumen - Pub - Current Hospital Medicine Quick Guide For Management of Common Medical Conditions in Acute Care Setting 1stnbspedDocument54 pagesDokumen - Pub - Current Hospital Medicine Quick Guide For Management of Common Medical Conditions in Acute Care Setting 1stnbspedMahmoud FathyNo ratings yet
- Hyponatremia (Essay)Document3 pagesHyponatremia (Essay)Wan HafizNo ratings yet
- Hyponatremia2010 (2014 - 09 - 24 18 - 08 - 47 UTC)Document181 pagesHyponatremia2010 (2014 - 09 - 24 18 - 08 - 47 UTC)rnsharmasNo ratings yet
- Diuretics 140628134114 Phpapp02Document45 pagesDiuretics 140628134114 Phpapp02P merugu100% (1)
- Mangement 2 PDFDocument165 pagesMangement 2 PDFjanveeNo ratings yet
- Volume and Tonicity DisordersDocument140 pagesVolume and Tonicity Disordersqbank.orgNo ratings yet
- Metabolic and Endocrine ManagementDocument42 pagesMetabolic and Endocrine ManagementAlyssa MontimorNo ratings yet
- LaCharity Practice Questions NclexDocument134 pagesLaCharity Practice Questions NclexKristen Nate100% (3)
- Body Fluids: Course: Physiology Prepared by Dr. A. Chebotarova, MD, PHDDocument61 pagesBody Fluids: Course: Physiology Prepared by Dr. A. Chebotarova, MD, PHDPreeti SharmaNo ratings yet
- Endocrine Pathophysiology Nursing Notes - Part 2Document10 pagesEndocrine Pathophysiology Nursing Notes - Part 2grad_nurse_2015100% (1)
- Screenshot 2021-06-23 at 11.36.48 AMDocument116 pagesScreenshot 2021-06-23 at 11.36.48 AMSmitha ShekarNo ratings yet
- 60 91 EndocrineDocument34 pages60 91 EndocrineYaj CruzadaNo ratings yet
- 06 and 07 HyponatremiaDocument68 pages06 and 07 HyponatremiaJoel TopfNo ratings yet
- Renal 3 - Regulation of Body Fluid Vol and Fluid OsmolarityDocument8 pagesRenal 3 - Regulation of Body Fluid Vol and Fluid OsmolarityManci Bito-onNo ratings yet
- Diabetes Insipidus and SIADH Reference Sheet: Normal Lab Values Siadh DIDocument13 pagesDiabetes Insipidus and SIADH Reference Sheet: Normal Lab Values Siadh DIJohn TusselNo ratings yet
- Pathophysiology Test Bank CH 18-19 & 21-22Document47 pagesPathophysiology Test Bank CH 18-19 & 21-22Joyy100% (5)