You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Suspected Neurological Conditions Recognition and Referral PDF 66141663923653Document76 pagesSuspected Neurological Conditions Recognition and Referral PDF 66141663923653Alex GasnasNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Facial Pain: Neurological and Non-Neurological: Joanna M ZakrzewskaDocument6 pagesFacial Pain: Neurological and Non-Neurological: Joanna M ZakrzewskaAlex GasnasNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Neuropathic Orofacial Pain Patients in Need of Dental Care: Jcda JadcDocument7 pagesNeuropathic Orofacial Pain Patients in Need of Dental Care: Jcda JadcAlex GasnasNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Orofacial Pain - An Update On Diagnosis and Management: PracticeDocument9 pagesOrofacial Pain - An Update On Diagnosis and Management: PracticeAlex GasnasNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Hypoglosal Nerve PalsyDocument4 pagesHypoglosal Nerve PalsyAlex GasnasNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Freemasonry Uncovering FreemasonryDocument113 pagesFreemasonry Uncovering Freemasonrycigsas1719100% (1)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- MITOCW - MIT9 - 00SCF11 - Lec20 - 300k.mp4: ProfessorDocument25 pagesMITOCW - MIT9 - 00SCF11 - Lec20 - 300k.mp4: ProfessorAlex GasnasNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Post-Ischemic in Ammation in The Brain: Takashi Shichita, Ryota Sakaguchi, Mayu Suzuki and Akihiko YoshimuraDocument7 pagesPost-Ischemic in Ammation in The Brain: Takashi Shichita, Ryota Sakaguchi, Mayu Suzuki and Akihiko YoshimuraAlex GasnasNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Death PathologyDocument80 pagesDeath PathologyAlex GasnasNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Funke Et Al-2011-The Journal of PhysiologyDocument13 pagesFunke Et Al-2011-The Journal of PhysiologyAlex GasnasNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- 2150 FullDocument7 pages2150 FullAlex GasnasNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- "Non-Invasive" Brain Stimulation Is Not Non-Invasive: Systems NeuroscienceDocument4 pages"Non-Invasive" Brain Stimulation Is Not Non-Invasive: Systems NeuroscienceAlex GasnasNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- CNS Other Infections: Pediatric Critical Care Medicine Emory University Children's Healthcare of AtlantaDocument70 pagesCNS Other Infections: Pediatric Critical Care Medicine Emory University Children's Healthcare of AtlantaAlex GasnasNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
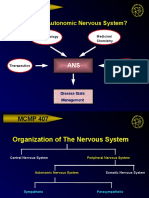
- MCMP 407: Why Study The Autonomic Nervous System?Document15 pagesMCMP 407: Why Study The Autonomic Nervous System?Alex GasnasNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- SIAC-2021-134 - Utah DMI Fentanyl ReportDocument27 pagesSIAC-2021-134 - Utah DMI Fentanyl ReportJeremy HarrisNo ratings yet
- Pediatricpainmanagement: Aarti Gaglani,, Toni GrossDocument12 pagesPediatricpainmanagement: Aarti Gaglani,, Toni GrossCarlos Manuel EscolasticoNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Methadone - DrugBankDocument13 pagesMethadone - DrugBankravaNo ratings yet
- Top 200 Brand Name DrugsDocument1 pageTop 200 Brand Name DrugsLen HuaNo ratings yet
- Pain NotesDocument4 pagesPain Notesrazelgc100% (4)
- Rectal Sedation: Chapter OutlineDocument5 pagesRectal Sedation: Chapter OutlinepoonpatchaNo ratings yet
- Care at The Time of DeathDocument11 pagesCare at The Time of DeathmultiusosvariadosNo ratings yet
- WalshcDocument26 pagesWalshcapi-530445129No ratings yet
- Guymer Giant Cell Arteritis Polymyalgia Rheumatica FibromyalgiaDocument93 pagesGuymer Giant Cell Arteritis Polymyalgia Rheumatica FibromyalgiaKe Xu100% (1)
- WHO Analgesic LadderDocument2 pagesWHO Analgesic LadderAndi PakdheeNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Drug Study ShenDocument12 pagesDrug Study ShenLass KazeNo ratings yet
- Determine of Morphine and Codeine in Human Urine by Gas Chromatography-Mass SpectrometryDocument7 pagesDetermine of Morphine and Codeine in Human Urine by Gas Chromatography-Mass Spectrometryamaliahriskaika100% (1)
- RAPIFEN AlfentanilDocument5 pagesRAPIFEN AlfentanilivankostadinovNo ratings yet
- Over The Counter DrugsDocument28 pagesOver The Counter DrugsManjusha KondepudiNo ratings yet
- AnalgesicDocument47 pagesAnalgesicMOHAMAD ZULFIKRIE ABASNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Current Issues in Spinal AnesthesiaDocument19 pagesCurrent Issues in Spinal AnesthesiaNadhifah RahmawatiNo ratings yet
- Case Study MyomaDocument18 pagesCase Study MyomaAgnes Nadine J. FraginalNo ratings yet
- Oklahoma Commission On Opioid Abuse Final ReportDocument12 pagesOklahoma Commission On Opioid Abuse Final ReportOKCFOXNo ratings yet
- Principles of Adolescent Substance Use Disorder TreatmentDocument42 pagesPrinciples of Adolescent Substance Use Disorder TreatmentDR DAN PEZZULO100% (2)
- Lesson 2 Drug Addiction and DependenceDocument24 pagesLesson 2 Drug Addiction and DependenceKen Kyle DavidNo ratings yet
- Northern Health - Overdose Prevention Services in Fort St. John and FAQs November 21, 2023Document8 pagesNorthern Health - Overdose Prevention Services in Fort St. John and FAQs November 21, 2023Tom SummerNo ratings yet
- Ketamine - What'S Old Is New Again: Mary Wojnakowski, Crna, PHD Director Nurse Anesthesia Program Midwestern UniversityDocument45 pagesKetamine - What'S Old Is New Again: Mary Wojnakowski, Crna, PHD Director Nurse Anesthesia Program Midwestern UniversityHendra HermawanNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Pharmacology NotesDocument30 pagesPharmacology NotesJessica WalkerNo ratings yet
- 2020.07.08.opp To Apportionment - MEMORANDUM - OF - LAW - I - 7212Document24 pages2020.07.08.opp To Apportionment - MEMORANDUM - OF - LAW - I - 7212Michael ReismanNo ratings yet
- Grant ProposalDocument4 pagesGrant Proposalapi-278415457No ratings yet
- Suicide and Types of Suicide Behavior Introduction To SuicideDocument107 pagesSuicide and Types of Suicide Behavior Introduction To SuicideMini Cooking EscapadeNo ratings yet
- Factors Influencing PainDocument81 pagesFactors Influencing Painlorella_abejuelaNo ratings yet
- Oral Drug Delivery 07Document28 pagesOral Drug Delivery 07Yuppie RajNo ratings yet
- Drug ListDocument18 pagesDrug ListMinh PhungNo ratings yet