You might also like
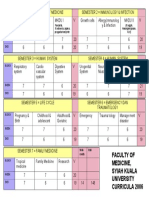
- Faculty of Medicine, Syiah Kuala University Curricula 2006Document1 pageFaculty of Medicine, Syiah Kuala University Curricula 2006wirdahajaNo ratings yet
- DIG Trauma HeparDocument37 pagesDIG Trauma HeparwirdahajaNo ratings yet
- Metabolic EncephalopathyDocument26 pagesMetabolic Encephalopathywirdahaja100% (3)
- Tinea UnguiumDocument8 pagesTinea UnguiumwirdahajaNo ratings yet
- Atopic DermatitisDocument19 pagesAtopic DermatitiswirdahajaNo ratings yet
- Microbiology - Scabies and PediculosisDocument32 pagesMicrobiology - Scabies and PediculosiswirdahajaNo ratings yet
- IRIS Retina ExplanationsDocument19 pagesIRIS Retina ExplanationsBalraj GangadharNo ratings yet
- TOEFL TEST Dan Kunci JawabanDocument5 pagesTOEFL TEST Dan Kunci JawabanwirdahajaNo ratings yet
- Diagnosis Banding Berbak Merah Kulit dan Diagnosis DifferensialDocument7 pagesDiagnosis Banding Berbak Merah Kulit dan Diagnosis DifferensialHari PranotoNo ratings yet
- Diagnosis Banding Berbak Merah Kulit dan Diagnosis DifferensialDocument7 pagesDiagnosis Banding Berbak Merah Kulit dan Diagnosis DifferensialHari PranotoNo ratings yet
- ABSES HATI-SytDocument29 pagesABSES HATI-SytwirdahajaNo ratings yet
- Cole StasisDocument59 pagesCole StasiswirdahajaNo ratings yet
- Metabolic EncephalopathyDocument26 pagesMetabolic Encephalopathywirdahaja100% (3)
- Anatomy of The Ear HearingDocument14 pagesAnatomy of The Ear HearingwirdahajaNo ratings yet
- Managing Abdominal Pain: A Guide for Diagnosis and TreatmentDocument38 pagesManaging Abdominal Pain: A Guide for Diagnosis and TreatmentSusi Muharni RismaNo ratings yet
- Defense Mechanism (IB)Document60 pagesDefense Mechanism (IB)wirdahajaNo ratings yet
- Clinical PathwayDocument154 pagesClinical Pathwaywirdahaja100% (1)
- Fever and RashDocument14 pagesFever and RashwirdahajaNo ratings yet
- Follow Up: No Tanggal Subjektif Objektif Assessment Planning TerapiDocument4 pagesFollow Up: No Tanggal Subjektif Objektif Assessment Planning TerapiwirdahajaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Guide to Cardiac Exam Findings and DiagnosesDocument58 pagesGuide to Cardiac Exam Findings and Diagnoseseliaszavaleta100% (1)
- Ventricular Assist DeviceDocument12 pagesVentricular Assist DevicesamadonyNo ratings yet
- ACC Cardiovascular Board Review MCQ 2017Document64 pagesACC Cardiovascular Board Review MCQ 2017Adeel Lakhiar100% (1)
- 2003-2013 March June FCPS Part 1 PapersDocument1,430 pages2003-2013 March June FCPS Part 1 Papersmoizzafar999No ratings yet
- Krok 2 2012-2019Document59 pagesKrok 2 2012-2019Donya GholamiNo ratings yet
- Pathophysiology Congenital Heart Disease-1Document54 pagesPathophysiology Congenital Heart Disease-1single_ladyNo ratings yet
- 2010 BasicDocument536 pages2010 Basicskypilot1433No ratings yet
- ECHO MASTERCLASS: A GUIDE TO ACCURATELY ASSESSING HEART VALVE DISEASEDocument136 pagesECHO MASTERCLASS: A GUIDE TO ACCURATELY ASSESSING HEART VALVE DISEASEVladlena Cucoș-CaraimanNo ratings yet
- Medicine MCQS JULY 2023 SOLVEDDocument15 pagesMedicine MCQS JULY 2023 SOLVEDLijo JoNo ratings yet
- Nbme Review Q'S - Fa2022-2023Document26 pagesNbme Review Q'S - Fa2022-2023poolada35No ratings yet
- Sample Review Questions in Medical and Surgical Nursing and Sample Board Exam QuestionsDocument22 pagesSample Review Questions in Medical and Surgical Nursing and Sample Board Exam Questionstinea nigraNo ratings yet
- Cardiothoracic SurgeryDocument24 pagesCardiothoracic SurgeryMARTINNo ratings yet
- Clinical QuidDocument175 pagesClinical QuidHassan Al SinanNo ratings yet
- Geriatric Medicine CasesDocument311 pagesGeriatric Medicine CasesShahnaaz Shah100% (7)
- Cardio NotesDocument7 pagesCardio Notesapi-3744683100% (4)
- Patho Cheat SheetDocument18 pagesPatho Cheat SheetJaney T.No ratings yet
- Gen Pathology CasesDocument41 pagesGen Pathology Casesrjh18950% (1)
- Board 14 Desember 2014 Kumpulan FinalDocument73 pagesBoard 14 Desember 2014 Kumpulan FinalAnonymous XHguqDfWR0% (1)
- Dissertation CardiologyDocument4 pagesDissertation CardiologyPaperWriterLowell100% (1)
- Sle PaperDocument73 pagesSle PaperRight VentricleNo ratings yet
- Apexocardiograma Precizari PracticeDocument12 pagesApexocardiograma Precizari PracticeDaniel VelciuNo ratings yet
- Anesthesia Guide for Mitral Stenosis PatientDocument67 pagesAnesthesia Guide for Mitral Stenosis PatientNamithaNo ratings yet
- Valvular Heart Disease Medical Surgical NursingDocument75 pagesValvular Heart Disease Medical Surgical NursingGodfrey Franco88% (8)
- 7th Heart Sounds and MurmursDocument6 pages7th Heart Sounds and MurmursbabibubeboNo ratings yet
- Chapter 28: Management of Patients With Structural, Infectious, and Inflammatory Cardiac DisordersDocument19 pagesChapter 28: Management of Patients With Structural, Infectious, and Inflammatory Cardiac DisordersBrian BileckyNo ratings yet
- Angised 90Document8 pagesAngised 90Darwesh FaqeerNo ratings yet
- Pathology of HEART - 1Document175 pagesPathology of HEART - 1Abdukadir AzamNo ratings yet
- Hypertrophic Cardiomyopathy: Joisy Aloor Leonard Shaju Smit Bhaisare Shawn RyneDocument36 pagesHypertrophic Cardiomyopathy: Joisy Aloor Leonard Shaju Smit Bhaisare Shawn RyneJoisy Aloor100% (1)
- AtacandDocument30 pagesAtacandAnna KowalskaNo ratings yet
- DR - Azad A Haleem AL - Brefkani: University of Duhok Faculty of Medical Science School of Medicine Pediatrics DepartmentDocument58 pagesDR - Azad A Haleem AL - Brefkani: University of Duhok Faculty of Medical Science School of Medicine Pediatrics DepartmentGomathi ShankarNo ratings yet