You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Psychodynamic Treatment of Depression PDFDocument420 pagesPsychodynamic Treatment of Depression PDFDelia Dascalu100% (1)
- Anxiety Depression Handbook-2Document44 pagesAnxiety Depression Handbook-2api-202351147No ratings yet
- Rorschach Interpretation Susan HimelsteinDocument51 pagesRorschach Interpretation Susan Himelsteindaniel serraniNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Bipolar Disorder Case StudyDocument10 pagesBipolar Disorder Case Studyapi-546243546No ratings yet
- Vagus Nerve StimulationDocument17 pagesVagus Nerve StimulationRicardo VillegasNo ratings yet
- (Medical Psychiatry 29) Borwin Bandelow, Dan J. Stein - Social Anxiety Disorder-Marcel Dekker (2004) PDFDocument347 pages(Medical Psychiatry 29) Borwin Bandelow, Dan J. Stein - Social Anxiety Disorder-Marcel Dekker (2004) PDFmaria100% (1)
- Lyme NeurotoxinsDocument46 pagesLyme NeurotoxinsJohnny Atman100% (1)
- Bipolar Affective Disorder, Current Manic Episode With Symptoms of Psychotic and Care in NursingDocument4 pagesBipolar Affective Disorder, Current Manic Episode With Symptoms of Psychotic and Care in NursingKit LaraNo ratings yet
- Dementia Care. Part 2 Understanding and Managing Behavioural ChallengesDocument7 pagesDementia Care. Part 2 Understanding and Managing Behavioural Challengesdogstar23100% (2)
- Clark PDFDocument8 pagesClark PDFEuge López RuizNo ratings yet
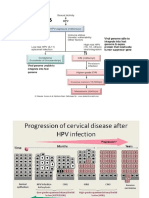
- Cervical Cancer YoDocument3 pagesCervical Cancer YoSafirahNo ratings yet
- Lipoma Removal GuideDocument2 pagesLipoma Removal GuideSteve D'HamsNo ratings yet
- Vocabulary List from English LessonDocument3 pagesVocabulary List from English LessonSafirahNo ratings yet
- Care of The Dying AIDS PatientsDocument53 pagesCare of The Dying AIDS PatientsSafirahNo ratings yet
- Vocabulary List from English LessonDocument3 pagesVocabulary List from English LessonSafirahNo ratings yet
- OT Medical Legal Reports - FLYERDocument1 pageOT Medical Legal Reports - FLYERSafirahNo ratings yet
- Seminar Written and Presented by Angela Price-Stephens - Publications - Presentation MaterialsDocument17 pagesSeminar Written and Presented by Angela Price-Stephens - Publications - Presentation MaterialsSafirahNo ratings yet
- Write Visum Et RepertumDocument3 pagesWrite Visum Et RepertumSafirahNo ratings yet
- Visum Et RepertumDocument5 pagesVisum Et RepertumSafirahNo ratings yet
- Nursing Interventions for Self-Care Deficit and DepressionDocument3 pagesNursing Interventions for Self-Care Deficit and DepressionDanica Kate GalleonNo ratings yet
- Teenage Depression Thesis StatementDocument7 pagesTeenage Depression Thesis Statementaimeebrowngilbert100% (2)
- Christine TayDocument15 pagesChristine TayTay TingNo ratings yet
- Texas Health Care Claims Study - Special Report On Foster Children, Strayhorn 2006Document294 pagesTexas Health Care Claims Study - Special Report On Foster Children, Strayhorn 2006Rick ThomaNo ratings yet
- Leeds Mental Health Needs Assessment 2011Document99 pagesLeeds Mental Health Needs Assessment 2011rob589100% (1)
- Research On Psychotherapy Efficacy and EffectivenessDocument18 pagesResearch On Psychotherapy Efficacy and EffectivenesspsicandreiaNo ratings yet
- Compare and Contrast Essay Example For Middle SchoolDocument4 pagesCompare and Contrast Essay Example For Middle Schoolafibyrirmfogiz100% (1)
- Abnormal PsychologyWEEKLY NOTESDocument73 pagesAbnormal PsychologyWEEKLY NOTESMelanie WaltersNo ratings yet
- Psychiatry Midterm Platings CompilationDocument8 pagesPsychiatry Midterm Platings CompilationicNo ratings yet
- People who experienced sleep paralysisDocument7 pagesPeople who experienced sleep paralysisAva BarramedaNo ratings yet
- Psychiatry Notes - Kaplan Vids, QuestionsDocument34 pagesPsychiatry Notes - Kaplan Vids, Questionskabal321No ratings yet
- USPSTF A and B Recommendations: Topic Description GradeDocument3 pagesUSPSTF A and B Recommendations: Topic Description GradeSantiago AldayNo ratings yet
- BP I Case StudyDocument29 pagesBP I Case StudyJoy-Rena Sabinay OchondraNo ratings yet
- What Is The Definition of InsomniaDocument24 pagesWhat Is The Definition of InsomniaHaniv Prasetya AdhiNo ratings yet
- Bipolar Disorder & Depression: Understanding the LinkDocument17 pagesBipolar Disorder & Depression: Understanding the LinkHasan Ahmed KhanNo ratings yet
- Week 1-3 ReadingsDocument115 pagesWeek 1-3 ReadingsJordan ZhengNo ratings yet
- Donali Lalich Literature ReviewDocument4 pagesDonali Lalich Literature Reviewapi-519746057No ratings yet
- CIRSG Manual EDocument30 pagesCIRSG Manual EBryanJermyHendrikNo ratings yet
- Atomoxetine in ADHD in Children With and Without Comorbid Mood DisordersDocument10 pagesAtomoxetine in ADHD in Children With and Without Comorbid Mood DisordersNeuro GYMNo ratings yet
- Learning Process-Based Therapy CAP 1Document8 pagesLearning Process-Based Therapy CAP 1Leidy PinzonNo ratings yet