You might also like
- JNC 8 Guideline Algorithm for Treating HypertensionDocument2 pagesJNC 8 Guideline Algorithm for Treating HypertensionTaradifaNurInsi0% (1)
- The Impaired of Renal, Heart and LiverDocument13 pagesThe Impaired of Renal, Heart and LiverRizki Khoirun HafidahNo ratings yet
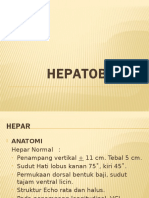
- HEPATOBILLIER: A CONCISE GUIDE TO LIVER AND GALLBLADDER ULTRASOUNDDocument45 pagesHEPATOBILLIER: A CONCISE GUIDE TO LIVER AND GALLBLADDER ULTRASOUNDRizki Khoirun HafidahNo ratings yet
- Translatean DR TaufikDocument9 pagesTranslatean DR TaufikRizki Khoirun HafidahNo ratings yet
- HEPATOBILLIER: A CONCISE GUIDE TO LIVER AND GALLBLADDER ULTRASOUNDDocument45 pagesHEPATOBILLIER: A CONCISE GUIDE TO LIVER AND GALLBLADDER ULTRASOUNDRizki Khoirun HafidahNo ratings yet
- NEURORADIOLOGY - SPINE IMAGINGDocument42 pagesNEURORADIOLOGY - SPINE IMAGINGRizki Khoirun HafidahNo ratings yet
- Non Hodgkin LimfomaDocument41 pagesNon Hodgkin LimfomaRizki Khoirun HafidahNo ratings yet
- Jurnal Gangguan Fungsi Ginjal, Jantung Dan HatiDocument6 pagesJurnal Gangguan Fungsi Ginjal, Jantung Dan HatiRizki Khoirun HafidahNo ratings yet
- Translatean DR TaufikDocument9 pagesTranslatean DR TaufikRizki Khoirun HafidahNo ratings yet
- NEURORADIOLOGY - SPINE IMAGINGDocument42 pagesNEURORADIOLOGY - SPINE IMAGINGRizki Khoirun HafidahNo ratings yet
- Evidence Quality for Periodic Health ExamsDocument3 pagesEvidence Quality for Periodic Health ExamsRizki Khoirun HafidahNo ratings yet
- Critical Appraisal ExperimentDocument9 pagesCritical Appraisal ExperimentArum Ardisa RiniNo ratings yet
- Critical Therapy Study ResultsDocument4 pagesCritical Therapy Study ResultsAinur 'iin' RahmahNo ratings yet
- E BM DiagnosisDocument12 pagesE BM DiagnosisArum Ardisa RiniNo ratings yet
- Critical Therapy Study ResultsDocument4 pagesCritical Therapy Study ResultsAinur 'iin' RahmahNo ratings yet
- Diagnostic Appraisal Sheet 2005Document3 pagesDiagnostic Appraisal Sheet 2005flatmajor7No ratings yet
- The Principal of ShockDocument18 pagesThe Principal of ShockRizki Khoirun HafidahNo ratings yet
- Diagnostic Appraisal Sheet 2005Document3 pagesDiagnostic Appraisal Sheet 2005flatmajor7No ratings yet
- The Principal of ShockDocument18 pagesThe Principal of ShockRizki Khoirun HafidahNo ratings yet
- The Principal of ShockDocument18 pagesThe Principal of ShockRizki Khoirun HafidahNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- SerfojiDocument58 pagesSerfojidarkknight2809No ratings yet
- Profile PDFDocument3 pagesProfile PDFsavan anvekarNo ratings yet
- Task 13 Eha Huwaida HayatiDocument3 pagesTask 13 Eha Huwaida HayatiEha Huwaida HayatiNo ratings yet
- Emergency Drug ListDocument17 pagesEmergency Drug ListLala Rahma Qodriyan SofiakmiNo ratings yet
- Premature Rupture of The MembraneDocument27 pagesPremature Rupture of The MembranezizsatriaNo ratings yet
- Nursing Bullets Fundamentals GuideDocument89 pagesNursing Bullets Fundamentals GuideJek NevadoNo ratings yet
- Cobas 8000 BrochureDocument20 pagesCobas 8000 BrochureRadu Badoiu100% (1)
- Gi BleedDocument33 pagesGi BleedMuhammad ArmghanNo ratings yet
- Music Intervention For Pain and AnxietyDocument37 pagesMusic Intervention For Pain and AnxietyVebryana RamadhaniaNo ratings yet
- Empyema ThoracisDocument33 pagesEmpyema ThoracisGracia EvangelistaNo ratings yet
- Female Urethral Cavernous Hemangioma, A Rare EntityDocument3 pagesFemale Urethral Cavernous Hemangioma, A Rare EntityAndre GunawanNo ratings yet
- Reflexology Research PapersDocument10 pagesReflexology Research Paperskyle atienzaNo ratings yet
- Puberty - GirlsDocument37 pagesPuberty - Girlsjonathan100% (1)
- Practical Medical Oncology Textbook (Antonio Russo, Marc Peeters, Lorena Incorvaia Etc.)Document1,104 pagesPractical Medical Oncology Textbook (Antonio Russo, Marc Peeters, Lorena Incorvaia Etc.)Paolo FassinaNo ratings yet
- Matary Cases 2013Document153 pagesMatary Cases 2013Raouf Ra'fat Soliman100% (10)
- Recent Advances in Endodontics Exploring The Trends in DiagnosisDocument4 pagesRecent Advances in Endodontics Exploring The Trends in DiagnosisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- BreechDocument50 pagesBreechEldrinAbquinaNo ratings yet
- Advanced Training in Nephrology Handbook 2019 20Document24 pagesAdvanced Training in Nephrology Handbook 2019 20Ashraf IsmailNo ratings yet
- @medicalbookpdf Preeclampsia PDFDocument286 pages@medicalbookpdf Preeclampsia PDFgalihsupanji111_2230No ratings yet
- Report On The Hospital VisitDocument4 pagesReport On The Hospital VisitSolanki PrakashNo ratings yet
- Synopsis TopicsDocument19 pagesSynopsis TopicsAbhishekNo ratings yet
- Rhinoplasty Dissection ManualDocument185 pagesRhinoplasty Dissection ManualVikas Vats100% (3)
- Lesson Plan On CataractDocument8 pagesLesson Plan On Cataractsimonjosan88% (8)
- Shierhana Awali Arasa: Trainings & SeminarsDocument2 pagesShierhana Awali Arasa: Trainings & SeminarsShierhana Awali ArasaNo ratings yet
- Jurnal On Hand SurgeryDocument187 pagesJurnal On Hand SurgeryMuhammad RezaNo ratings yet
- ACS BookletDocument14 pagesACS Bookletmyat25No ratings yet
- Anna Eakes - Reflection PaperDocument7 pagesAnna Eakes - Reflection Paperapi-558091839No ratings yet
- Stockard Tests UE & LE TDocument4 pagesStockard Tests UE & LE TLinh HoangNo ratings yet
- Daftar Pustaka: Selma Mutiara Hani, Dr. Moh Nailul Fahmi, SP - OG Dr. Fatwa Sari Tetra Dewi, MPH., PH.DDocument10 pagesDaftar Pustaka: Selma Mutiara Hani, Dr. Moh Nailul Fahmi, SP - OG Dr. Fatwa Sari Tetra Dewi, MPH., PH.DRohadatul Aisy Kurnia PutriNo ratings yet
- Practice Standards For Midwives 2015Document28 pagesPractice Standards For Midwives 2015graceNo ratings yet