You might also like
- Breaking the Chains of Diabetes. A Comprehensive Guide to Understanding and Managing Diabetes NaturallyFrom EverandBreaking the Chains of Diabetes. A Comprehensive Guide to Understanding and Managing Diabetes NaturallyNo ratings yet
- Practical Insulin: A Handbook for Prescribing ProvidersFrom EverandPractical Insulin: A Handbook for Prescribing ProvidersRating: 5 out of 5 stars5/5 (2)
- Insulin PharmacologyDocument4 pagesInsulin PharmacologySunilNo ratings yet
- What Is Diabetes, Its Types, Role of Insulin and Hypoglycemic Agents, Mode of Action, Side Effects, Pharmacodynamics and PharmacokineticsDocument9 pagesWhat Is Diabetes, Its Types, Role of Insulin and Hypoglycemic Agents, Mode of Action, Side Effects, Pharmacodynamics and PharmacokineticsIshaani GargNo ratings yet
- Drugs of DiabetesDocument42 pagesDrugs of Diabeteskwennybiang100% (1)
- Diabetes Mellitus (DM) : ContentDocument30 pagesDiabetes Mellitus (DM) : ContentMompati LetsweletseNo ratings yet
- Diabetes PharmacologyDocument14 pagesDiabetes PharmacologyRich JeongNo ratings yet
- Lewis: Medical-Surgical Nursing, 10 Edition: Diabetes Mellitus Key PointsDocument6 pagesLewis: Medical-Surgical Nursing, 10 Edition: Diabetes Mellitus Key PointsDeo FactuarNo ratings yet
- Drug Management of Diabetes MellitusDocument36 pagesDrug Management of Diabetes MellitusHassan.shehri100% (15)
- Insulin and Antidiabetic Drugs: Prof - DR Asya RehmanDocument23 pagesInsulin and Antidiabetic Drugs: Prof - DR Asya RehmanGareth BaleNo ratings yet
- Pharmacotherapy of Diabetes MellitusDocument32 pagesPharmacotherapy of Diabetes MellitusGhilli Jaya PrakashNo ratings yet
- Treatment of Diabetes MellitusDocument31 pagesTreatment of Diabetes MellitusIrfan IdealistNo ratings yet
- Antidiabetic Drugs. Nurse 2024Document32 pagesAntidiabetic Drugs. Nurse 2024Ayro Business CenterNo ratings yet
- ANTIDIABETICSDocument25 pagesANTIDIABETICSkookiescream100% (2)
- LEC#37 Anti Diabetic Drugs (Insulin)Document20 pagesLEC#37 Anti Diabetic Drugs (Insulin)alihyderabro166No ratings yet
- Oral Management of Diabetes Type IIDocument34 pagesOral Management of Diabetes Type IIYasser Gebril100% (1)
- Antidiabetic DrugsDocument68 pagesAntidiabetic DrugsninetysevenccNo ratings yet
- Drugs For Diabetes (Part 1)Document6 pagesDrugs For Diabetes (Part 1)حوراء عارف الموسويNo ratings yet
- Second 7 PharmaDocument17 pagesSecond 7 PharmaHassan TantawyNo ratings yet
- Oral HypoglycemicDocument5 pagesOral HypoglycemicDavid HosamNo ratings yet
- Diabetes Mellitus Type 2Document42 pagesDiabetes Mellitus Type 2alexandrajane2007No ratings yet
- Oral Antidiabetic AgentsDocument4 pagesOral Antidiabetic AgentsFendi Ali100% (1)
- Endo Pharma ElhDocument14 pagesEndo Pharma Elhodiodi57No ratings yet
- Classifications of Insulin2Document116 pagesClassifications of Insulin2loglesb1No ratings yet
- 5th WS-DM 02Document38 pages5th WS-DM 02Andy F MonroeNo ratings yet
- Oral HypoglycemicsDocument50 pagesOral HypoglycemicsSudhakar LakavathNo ratings yet
- Pancreatic Hormones Antidiabetic Drugs Part 2Document24 pagesPancreatic Hormones Antidiabetic Drugs Part 2jenet soleilNo ratings yet
- Ix. Drug Study: Drug Name Action Indication Contraindication Adverse Effect Nursing ResponsibilitiesDocument2 pagesIx. Drug Study: Drug Name Action Indication Contraindication Adverse Effect Nursing ResponsibilitiesKaloy AnneNo ratings yet
- Las-No 6Document44 pagesLas-No 6jenet soleilNo ratings yet
- Management of DMDocument9 pagesManagement of DMnurul izzatiNo ratings yet
- NRSE 3010 Chapter 47Document52 pagesNRSE 3010 Chapter 47Karina IvanchenkoNo ratings yet
- ANTI-DIABETIC AGENTS (OHAs)Document42 pagesANTI-DIABETIC AGENTS (OHAs)Prajwal Rao KNo ratings yet
- Pathophysiology and Management of Diabetes Mellitus GppqeDocument60 pagesPathophysiology and Management of Diabetes Mellitus GppqeOlivia OliverNo ratings yet
- Diabetes Farmacot Eleição 2018 Aust Prescriber Traduzir para PMVDocument4 pagesDiabetes Farmacot Eleição 2018 Aust Prescriber Traduzir para PMVElizoneth SessaNo ratings yet
- Welcome To The PresentationDocument32 pagesWelcome To The PresentationIshaan Arfatur Rahman0% (1)
- DM GeneralDocument39 pagesDM GeneralDr Sachin Patil100% (1)
- Diabetes MellitusDocument181 pagesDiabetes Mellitusnursereview95% (19)
- Antidiabetic Drugs: DR Nagwa Nour EL Din Assistant Professor PharmacologyDocument18 pagesAntidiabetic Drugs: DR Nagwa Nour EL Din Assistant Professor PharmacologyMohamed AlaaNo ratings yet
- Pharmacologic TheraphyDocument32 pagesPharmacologic TheraphyquinnNo ratings yet
- 11 - Diabetes MellitusDocument63 pages11 - Diabetes MellitusShady ChapookNo ratings yet
- Carlos D. Achondo Jr. 2MD-1 March 30, 2020Document4 pagesCarlos D. Achondo Jr. 2MD-1 March 30, 2020Carlos NiñoNo ratings yet
- Management of Diabetes Mellitus.: Dietary ModificationDocument1 pageManagement of Diabetes Mellitus.: Dietary ModificationAhmed Taha Abo ElnourNo ratings yet
- Pharmacotherapy of Diabetes Mellitus: Dr. Ave Olivia Rahman, Msc. Bagian Farmakologi Fkik UnjaDocument42 pagesPharmacotherapy of Diabetes Mellitus: Dr. Ave Olivia Rahman, Msc. Bagian Farmakologi Fkik UnjaGita Tanbao SuselinNo ratings yet
- Pancreatic Hormones Antidiabetic DrugsDocument69 pagesPancreatic Hormones Antidiabetic DrugsTâm MinhNo ratings yet
- Management of Diabetes Mellitus 11Document25 pagesManagement of Diabetes Mellitus 11khalid.zainabNo ratings yet
- 6 Intro To DMDocument38 pages6 Intro To DMSPUB HPONTIANNo ratings yet
- Diabetes MedicationDocument17 pagesDiabetes MedicationTaj lamajedNo ratings yet
- Pancreatic Hormones by KatzungDocument3 pagesPancreatic Hormones by KatzungChristian DeeNo ratings yet
- DM Presentation NewDocument44 pagesDM Presentation NewKipz JonsNo ratings yet
- 4 Oral Hypoglycaemic DrugsDocument10 pages4 Oral Hypoglycaemic DrugsNashat SaadiNo ratings yet
- Diabetic NephropathyDocument4 pagesDiabetic NephropathyroshmaeNo ratings yet
- Diabetes Mellitus: Salient Features of Type 1 Am D Type 2 DMDocument20 pagesDiabetes Mellitus: Salient Features of Type 1 Am D Type 2 DMPriyanka Karnik100% (1)
- Meglitinide Analogues Are Classified As Insulin Secretagogues and Have Actions andDocument6 pagesMeglitinide Analogues Are Classified As Insulin Secretagogues and Have Actions andRifqoh Aulia AlthofunnisaNo ratings yet
- Pharmacotherapy of DMDocument28 pagesPharmacotherapy of DMQueenElsaNo ratings yet
- Diabetes Mellitus - UG NotesDocument10 pagesDiabetes Mellitus - UG NotesRayan ElRasheedNo ratings yet
- 08&09 Oral Hypoglycemics-Level 11Document48 pages08&09 Oral Hypoglycemics-Level 11Usman Ali AkbarNo ratings yet
- FO-Antidiabetic-27042020-Blok 7Document64 pagesFO-Antidiabetic-27042020-Blok 7Indah NurhalizaNo ratings yet
- Endocrine 1677476082Document36 pagesEndocrine 1677476082Winhtut ThantNo ratings yet
- Type 2 DMDocument14 pagesType 2 DMraffia mehakNo ratings yet
- FR H 6788 001 FinalSPCDocument28 pagesFR H 6788 001 FinalSPCabenezer g/kirstosNo ratings yet
- Frequent Urination Case IDocument13 pagesFrequent Urination Case IironNo ratings yet
- Treatment Viral MeningitisDocument9 pagesTreatment Viral MeningitisironNo ratings yet
- SOP 36 Pemeriksaan Urine LengkapDocument3 pagesSOP 36 Pemeriksaan Urine LengkapSevy AyuayuNo ratings yet
- Pathophysiology of SeizuresDocument11 pagesPathophysiology of SeizuresironNo ratings yet
- Nephrogenic Diabetes Insipidus (Includes: Nephrogenic Diabetes Insipidus, Autosomal Nephrogenic Diabetes Insipidus, X-Linked)Document18 pagesNephrogenic Diabetes Insipidus (Includes: Nephrogenic Diabetes Insipidus, Autosomal Nephrogenic Diabetes Insipidus, X-Linked)ironNo ratings yet
- TREATMENT Bacterial MeningitisDocument32 pagesTREATMENT Bacterial MeningitisironNo ratings yet
- Case #3 (Macazo, Manueke, Purba) : CBC ResultsDocument2 pagesCase #3 (Macazo, Manueke, Purba) : CBC ResultsironNo ratings yet
- Diabetes MellitusDocument32 pagesDiabetes Mellitusiron100% (1)
- PregnacyDocument12 pagesPregnacyironNo ratings yet
- DM Labs TherapDocument54 pagesDM Labs TherapironNo ratings yet
- Diet RX Cal 2350kcal CHO 325g PRO 120g FAT 65gDocument4 pagesDiet RX Cal 2350kcal CHO 325g PRO 120g FAT 65gironNo ratings yet
- Mechanism of CoughDocument7 pagesMechanism of Coughiron100% (1)
- Diabetes Exchange ListDocument10 pagesDiabetes Exchange ListironNo ratings yet
- Acute Complication of DM: Clinical Manifestation Laboratory Procedures Therapeutic Plan Possible Problem AssociatedDocument12 pagesAcute Complication of DM: Clinical Manifestation Laboratory Procedures Therapeutic Plan Possible Problem AssociatedironNo ratings yet
- Pathology and Pathogenesis of CopdDocument19 pagesPathology and Pathogenesis of CopdironNo ratings yet
- Chronic Complications of Diabetes MellitusDocument40 pagesChronic Complications of Diabetes MellitusironNo ratings yet
- Chronic Complications of Diabetes MellitusDocument35 pagesChronic Complications of Diabetes MellitusironNo ratings yet
- Therapeutic Plan 4 Acute DMDocument21 pagesTherapeutic Plan 4 Acute DMironNo ratings yet
- Pancreas: - Anatomy and Histology - Normal Physiology of The Endocrine PancreasDocument34 pagesPancreas: - Anatomy and Histology - Normal Physiology of The Endocrine PancreasironNo ratings yet
- Etiopathogenesis of Diabetes MellitusDocument35 pagesEtiopathogenesis of Diabetes MellitusironNo ratings yet
- Medical History (Cough)Document3 pagesMedical History (Cough)ironNo ratings yet
- Mechanisms of Cough From AngiotensinDocument1 pageMechanisms of Cough From AngiotensinironNo ratings yet
- Initial Assessment: A Full History Is NeededDocument37 pagesInitial Assessment: A Full History Is NeededironNo ratings yet
- Type 1 Diabetes Mellitus: TreatmentDocument25 pagesType 1 Diabetes Mellitus: TreatmentironNo ratings yet
- Interpretation of Laboratory Tests: CBC Chest X-Ray ABG Sputum GsDocument5 pagesInterpretation of Laboratory Tests: CBC Chest X-Ray ABG Sputum GsironNo ratings yet
- GlucocorticoidsDocument9 pagesGlucocorticoidsironNo ratings yet
- GlucocorticoidsDocument9 pagesGlucocorticoidsironNo ratings yet
- EmphysemaDocument19 pagesEmphysemaironNo ratings yet
- Emphysema 1Document7 pagesEmphysema 1ironNo ratings yet
- Group DR - Script - Allergic Rhinitis (Peanut Allergy) Health EducationDocument10 pagesGroup DR - Script - Allergic Rhinitis (Peanut Allergy) Health EducationKyra Bianca R. FamacionNo ratings yet
- Chapter 2 Lesson 1Document3 pagesChapter 2 Lesson 1John Carldel VivoNo ratings yet
- Safety Pocket Guide Web 061808Document534 pagesSafety Pocket Guide Web 061808hombre911100% (1)
- Hazard Analysis in The WorkplaceDocument7 pagesHazard Analysis in The WorkplaceUghlahnNo ratings yet
- Food SafetyDocument2 pagesFood SafetymacmanueNo ratings yet
- FEDIAF Nutritional Guidelines 2020 20200917Document96 pagesFEDIAF Nutritional Guidelines 2020 20200917luciana ribeiroNo ratings yet
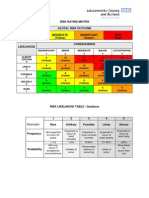
- Example of A NHS Risk Rating MatrixDocument2 pagesExample of A NHS Risk Rating MatrixRochady SetiantoNo ratings yet
- PARS 19 - Slide PDFDocument23 pagesPARS 19 - Slide PDFNorsyaliza Abd Razak100% (1)
- Extend XT - Folleto ComercialDocument6 pagesExtend XT - Folleto ComercialMuhamadZuhdiAlWaliNo ratings yet
- Disaster Nursing SAS Session 14Document6 pagesDisaster Nursing SAS Session 14Niceniadas CaraballeNo ratings yet
- Target Heart Rate Lesson PlanDocument4 pagesTarget Heart Rate Lesson PlanEryn YeskeNo ratings yet
- Nejmra 2023911Document8 pagesNejmra 2023911Merry LeeNo ratings yet
- Pappas Bikhazi 2023 Babe Ruth S Anaplastic Epidermoid Carcinoma of The NasopharynxDocument5 pagesPappas Bikhazi 2023 Babe Ruth S Anaplastic Epidermoid Carcinoma of The NasopharynxVinoster ProductionNo ratings yet
- Chapter 1 Principles of AssessmentDocument12 pagesChapter 1 Principles of Assessmentmupt77No ratings yet
- The Diagram Shows How A Company Called HB Office RDocument1 pageThe Diagram Shows How A Company Called HB Office RbugakNo ratings yet
- Anxiety Disorder by SlidesgoDocument55 pagesAnxiety Disorder by SlidesgoShey DraftsNo ratings yet
- The Effectiveness of Information System in Divine Mercy Hospitalsan Pedro LagunaDocument22 pagesThe Effectiveness of Information System in Divine Mercy Hospitalsan Pedro LagunamartNo ratings yet
- The Influence of Music in Horror Games (Final Draft)Document7 pagesThe Influence of Music in Horror Games (Final Draft)Panther LenoXNo ratings yet
- Recreational Water Quality Guidelines and Aesthetics - IntroductionDocument3 pagesRecreational Water Quality Guidelines and Aesthetics - IntroductionLenin Jorge Villanueva DuranNo ratings yet
- For DissertationDocument13 pagesFor DissertationRegi viniciyaNo ratings yet
- Gear Oil 85W-140: Safety Data SheetDocument7 pagesGear Oil 85W-140: Safety Data SheetsaadNo ratings yet
- Interpretative Phenomenological Analysis - AddictionDocument14 pagesInterpretative Phenomenological Analysis - AddictionAna MariaNo ratings yet
- Pro-Oxidant Strategies - Cancer Treatments ResearchDocument71 pagesPro-Oxidant Strategies - Cancer Treatments ResearchSpore FluxNo ratings yet
- Dibasic Sodium PhosphateDocument0 pagesDibasic Sodium PhosphateWilliam ChandraNo ratings yet
- The Impact of Longitudinal Studies On Understanding Development From Young Adulthood To Old AgeDocument11 pagesThe Impact of Longitudinal Studies On Understanding Development From Young Adulthood To Old AgeLana PeharNo ratings yet
- الصحة PDFDocument17 pagesالصحة PDFGamal MansourNo ratings yet
- Diana Barnett Course Critique n5327 RDocument4 pagesDiana Barnett Course Critique n5327 Rapi-308950624No ratings yet
- Pag-Unawa Sa Mga Panganib NG Sobrang Dosis NG Alkohol: Ano Ang Isang Pamantayang Tagay?Document5 pagesPag-Unawa Sa Mga Panganib NG Sobrang Dosis NG Alkohol: Ano Ang Isang Pamantayang Tagay?Rochelle Bartocillo BasquezNo ratings yet
- Thinking CriticallyDocument31 pagesThinking CriticallyAnonymous HU37mJ50% (2)
- Sensus Harian TGL 05 Maret 2022........Document104 pagesSensus Harian TGL 05 Maret 2022........Ruhut Putra SinuratNo ratings yet