You might also like
- Diabetes Part 1Document32 pagesDiabetes Part 1Zaid Al-KadhimiNo ratings yet
- 4DM PresentationDocument57 pages4DM Presentationamal nassarNo ratings yet
- Diabetes Mellitus IIDocument10 pagesDiabetes Mellitus IIaa zzNo ratings yet
- Endocrine CologyDocument124 pagesEndocrine CologyBehailu TejeNo ratings yet
- Diabetes Mellitus - UG NotesDocument10 pagesDiabetes Mellitus - UG NotesRayan ElRasheedNo ratings yet
- Drugs For Diabetes MellitusDocument50 pagesDrugs For Diabetes MellitusCherenet TomaNo ratings yet
- Treatment of Diabetes MellitusDocument25 pagesTreatment of Diabetes MellitusPurnima ChoudhuryNo ratings yet
- Antidiabetic Agents GuideDocument19 pagesAntidiabetic Agents GuideJames SoeNo ratings yet
- Recent Advances in Therapy of DiabetesDocument62 pagesRecent Advances in Therapy of DiabetesMohd KhatibNo ratings yet
- General Principles of Insulin Therapy in Diabetes MellitusDocument24 pagesGeneral Principles of Insulin Therapy in Diabetes MellitusEDWIN WIJAYANo ratings yet
- Drug Management of Diabetes MellitusDocument36 pagesDrug Management of Diabetes MellitusHassan.shehri100% (15)
- Insulin NewDocument41 pagesInsulin NewSheikNo ratings yet
- DM Lab 2 - FinalDocument33 pagesDM Lab 2 - FinalMahamed Wefkey OmranNo ratings yet
- General Principles of Insulin Therapy in Diabetes Mellitus - UpToDateDocument20 pagesGeneral Principles of Insulin Therapy in Diabetes Mellitus - UpToDateabdulghaniNo ratings yet
- Anti-Diabetic Drugs InsulinDocument26 pagesAnti-Diabetic Drugs Insulinwissam salimNo ratings yet
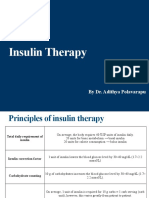
- Insulin Therapy: by Dr. Adithya PolavarapuDocument18 pagesInsulin Therapy: by Dr. Adithya Polavarapuadithya polavarapuNo ratings yet
- Insulin, Oral Hypoglycemic Agents-1Document23 pagesInsulin, Oral Hypoglycemic Agents-1IbrahimNo ratings yet
- Insulin Initiation and MonitoringDocument35 pagesInsulin Initiation and Monitoringeka prasepti darusmanNo ratings yet
- General Principles of Insulin Therapy in Diabetes MellitusDocument12 pagesGeneral Principles of Insulin Therapy in Diabetes MellitusRuban RichardNo ratings yet
- Antidiabetic Drugs. Nurse 2024Document32 pagesAntidiabetic Drugs. Nurse 2024Ayro Business CenterNo ratings yet
- Pharmacology Review NotesDocument24 pagesPharmacology Review NotescampbellqueenNo ratings yet
- Hayatt Univesity College. Faculty of Medicine. Family Medicine. Mohamed Gassim Mohamed. Insulin ManagementDocument14 pagesHayatt Univesity College. Faculty of Medicine. Family Medicine. Mohamed Gassim Mohamed. Insulin ManagementMohammed GassimNo ratings yet
- Long Term DiabetesDocument68 pagesLong Term Diabetesnawaraj2044No ratings yet
- Insulin & Oral Antidiabetic Drugs GuideDocument37 pagesInsulin & Oral Antidiabetic Drugs GuidePrithulNo ratings yet
- Insulin and Antidiabetic Drugs: Prof - DR Asya RehmanDocument23 pagesInsulin and Antidiabetic Drugs: Prof - DR Asya RehmanGareth BaleNo ratings yet
- Diabetes Study GuideDocument4 pagesDiabetes Study GuideNicole Brassington0% (1)
- InsulinDocument4 pagesInsulinHa Zizzle100% (1)
- Approsch To DM1Document4 pagesApprosch To DM1M MazloumNo ratings yet
- Diabetic DrugsDocument39 pagesDiabetic DrugsNONDUMISONo ratings yet
- All About Insulin: Jill E. Vollbrecht, MDDocument41 pagesAll About Insulin: Jill E. Vollbrecht, MDkeylapireNo ratings yet
- Diabetes Treatment: Dr. Chavan P.R. Pharm DDocument73 pagesDiabetes Treatment: Dr. Chavan P.R. Pharm DAvel ChandNo ratings yet
- Pharmacotherapy of Diabetes Mellitus: Dr. Ave Olivia Rahman, Msc. Bagian Farmakologi Fkik UnjaDocument42 pagesPharmacotherapy of Diabetes Mellitus: Dr. Ave Olivia Rahman, Msc. Bagian Farmakologi Fkik UnjaEya Prepti SerraNo ratings yet
- Drugs of DiabetesDocument42 pagesDrugs of Diabeteskwennybiang100% (1)
- Drugs That Affect The Endocrine SystemDocument75 pagesDrugs That Affect The Endocrine SystemTadela MengashaNo ratings yet
- Drugs Used to Treat Diabetes Mellitus: Insulin and Oral AgentsDocument37 pagesDrugs Used to Treat Diabetes Mellitus: Insulin and Oral AgentsjisooNo ratings yet
- Drugs For Diabetes (Part 1)Document6 pagesDrugs For Diabetes (Part 1)حوراء عارف الموسويNo ratings yet
- Antidiabetic Drugs: DR Nagwa Nour EL Din Assistant Professor PharmacologyDocument18 pagesAntidiabetic Drugs: DR Nagwa Nour EL Din Assistant Professor PharmacologyMohamed AlaaNo ratings yet
- Dietetik TerjemahDocument8 pagesDietetik TerjemahAsrori MuhofiNo ratings yet
- DM Presentation NewDocument44 pagesDM Presentation NewKipz JonsNo ratings yet
- Drugs Affecting Endocrine and Reproductive SystemDocument109 pagesDrugs Affecting Endocrine and Reproductive SystemJann ericka JaoNo ratings yet
- Insulin PharmDocument21 pagesInsulin PharmMeredith Barb0% (1)
- Dr.Rihab Pediatrics 02.Pediatric DM Part TwoDocument7 pagesDr.Rihab Pediatrics 02.Pediatric DM Part TwoMujtaba JawadNo ratings yet
- A Practical Guide To Insulin TherapyDocument42 pagesA Practical Guide To Insulin Therapyseun williams100% (2)
- Endocrine Pancreas PharmacologyDocument38 pagesEndocrine Pancreas PharmacologydarkmagicdrakeNo ratings yet
- DiabetesDocument42 pagesDiabetesSteph VistalNo ratings yet
- Insulin Clinician5 PharmacyDocument4 pagesInsulin Clinician5 PharmacydafaloveNo ratings yet
- Pharmacotherapy - Diabetes II - Dr. Mohammed KamalDocument46 pagesPharmacotherapy - Diabetes II - Dr. Mohammed KamalMohammed KamalNo ratings yet
- Pharmacotherapy of Diabetes Mellitus: Dr. Ave Olivia Rahman, Msc. Bagian Farmakologi Fkik UnjaDocument42 pagesPharmacotherapy of Diabetes Mellitus: Dr. Ave Olivia Rahman, Msc. Bagian Farmakologi Fkik UnjaGita Tanbao SuselinNo ratings yet
- DM Ppt. NewDocument26 pagesDM Ppt. NewRio Ramon HilarioNo ratings yet
- GUIDELINES FOR INPATIENT DIABETES MANAGEMENT هااامDocument1 pageGUIDELINES FOR INPATIENT DIABETES MANAGEMENT هااامAbu HuzaifaNo ratings yet
- Peran Perawat DLM Rawat Inap DMDocument57 pagesPeran Perawat DLM Rawat Inap DMMuhidin AeNo ratings yet
- Treatment of Diabetes MellitusDocument31 pagesTreatment of Diabetes MellitusIrfan IdealistNo ratings yet
- Anti-Diabetic Drugs GuideDocument39 pagesAnti-Diabetic Drugs GuideNurul Mursyidah ZakariaNo ratings yet
- Manejo de La DMGDocument5 pagesManejo de La DMGsandymejiaNo ratings yet
- Effective Use of Insulin Therapy in Type 2 DiabetesDocument7 pagesEffective Use of Insulin Therapy in Type 2 DiabetesmariohuangNo ratings yet
- Antidiabetic Agents: Diabetes MellitusDocument7 pagesAntidiabetic Agents: Diabetes MellitusRatika SariNo ratings yet
- Pancreatic Hormone & Antidiabetic Drugs: Renato I. Dalmacio, RPH Pharmacology 414 College of PharmacyDocument69 pagesPancreatic Hormone & Antidiabetic Drugs: Renato I. Dalmacio, RPH Pharmacology 414 College of PharmacyRalf EmoteroNo ratings yet
- Diabetic DrugDocument16 pagesDiabetic DrugAbu Sadat Md. SayemNo ratings yet
- Anti Diabetic DrugsDocument54 pagesAnti Diabetic Drugsmanj99No ratings yet
- Practical Insulin: A Handbook for Prescribing ProvidersFrom EverandPractical Insulin: A Handbook for Prescribing ProvidersRating: 5 out of 5 stars5/5 (2)
- Treatment Viral MeningitisDocument9 pagesTreatment Viral MeningitisironNo ratings yet
- TREATMENT Bacterial MeningitisDocument32 pagesTREATMENT Bacterial MeningitisironNo ratings yet
- Pathophysiology of SeizuresDocument11 pagesPathophysiology of SeizuresironNo ratings yet
- Diabetes MellitusDocument32 pagesDiabetes Mellitusiron100% (1)
- Acute Complication of DM: Clinical Manifestation Laboratory Procedures Therapeutic Plan Possible Problem AssociatedDocument12 pagesAcute Complication of DM: Clinical Manifestation Laboratory Procedures Therapeutic Plan Possible Problem AssociatedironNo ratings yet
- SOP 36 Pemeriksaan Urine LengkapDocument3 pagesSOP 36 Pemeriksaan Urine LengkapSevy AyuayuNo ratings yet
- Nephrogenic Diabetes Insipidus (Includes: Nephrogenic Diabetes Insipidus, Autosomal Nephrogenic Diabetes Insipidus, X-Linked)Document18 pagesNephrogenic Diabetes Insipidus (Includes: Nephrogenic Diabetes Insipidus, Autosomal Nephrogenic Diabetes Insipidus, X-Linked)ironNo ratings yet
- DIABETES EXCHANGE LISTSDocument10 pagesDIABETES EXCHANGE LISTSironNo ratings yet
- Frequent Urination Case StudyDocument13 pagesFrequent Urination Case StudyironNo ratings yet
- PregnacyDocument12 pagesPregnacyironNo ratings yet
- DM Labs TherapDocument54 pagesDM Labs TherapironNo ratings yet
- Weight, height, BMI and calorie needsDocument4 pagesWeight, height, BMI and calorie needsironNo ratings yet
- Therapeutic Plan 4 Acute DMDocument21 pagesTherapeutic Plan 4 Acute DMironNo ratings yet
- Chronic Complications of Diabetes MellitusDocument40 pagesChronic Complications of Diabetes MellitusironNo ratings yet
- Case #3 (Macazo, Manueke, Purba) : CBC ResultsDocument2 pagesCase #3 (Macazo, Manueke, Purba) : CBC ResultsironNo ratings yet
- COPD Treatment with Inhaled GlucocorticoidsDocument9 pagesCOPD Treatment with Inhaled GlucocorticoidsironNo ratings yet
- Managing Diabetes ComplicationsDocument35 pagesManaging Diabetes ComplicationsironNo ratings yet
- Etiopathogenesis of Diabetes MellitusDocument35 pagesEtiopathogenesis of Diabetes MellitusironNo ratings yet
- Mechanism of CoughDocument7 pagesMechanism of Coughiron100% (1)
- Pharmacological treatment for type 1 and type 2 diabetes mellitusDocument26 pagesPharmacological treatment for type 1 and type 2 diabetes mellitusiron100% (1)
- Comprehensive assessment and management plan for type 1 diabetesDocument37 pagesComprehensive assessment and management plan for type 1 diabetesironNo ratings yet
- Pancreas: - Anatomy and Histology - Normal Physiology of The Endocrine PancreasDocument34 pagesPancreas: - Anatomy and Histology - Normal Physiology of The Endocrine PancreasironNo ratings yet
- Pathology and Pathogenesis of CopdDocument19 pagesPathology and Pathogenesis of CopdironNo ratings yet
- Interpretation of Laboratory Tests: CBC Chest X-Ray ABG Sputum GsDocument5 pagesInterpretation of Laboratory Tests: CBC Chest X-Ray ABG Sputum GsironNo ratings yet
- Medical History (Cough)Document3 pagesMedical History (Cough)ironNo ratings yet
- COPD Treatment with Inhaled GlucocorticoidsDocument9 pagesCOPD Treatment with Inhaled GlucocorticoidsironNo ratings yet
- Mechanisms of Cough From AngiotensinDocument1 pageMechanisms of Cough From AngiotensinironNo ratings yet
- Emphysema 1Document7 pagesEmphysema 1ironNo ratings yet
- EmphysemaDocument19 pagesEmphysemaironNo ratings yet
- Diabetes Facts and Guidelines: en Te RDocument53 pagesDiabetes Facts and Guidelines: en Te Rroche_reyesNo ratings yet
- Levemir Product Insert PDFDocument11 pagesLevemir Product Insert PDFDegee O. GonzalesNo ratings yet
- Insulin in DMDocument46 pagesInsulin in DMask1400No ratings yet
- Estrategias Contra A Diabetes (170pag)Document170 pagesEstrategias Contra A Diabetes (170pag)vicenteNo ratings yet
- Insulin Detemir and Basal Insulin TherapyDocument7 pagesInsulin Detemir and Basal Insulin Therapymayrapp16No ratings yet
- Pancreatic Hormones & Antidiabetic Drugs: Case StudyDocument31 pagesPancreatic Hormones & Antidiabetic Drugs: Case StudyMae Lislie Canonigo - FloresNo ratings yet
- The Review of Medicines Used For Treating Diabetes: A SummaryDocument8 pagesThe Review of Medicines Used For Treating Diabetes: A SummaryAliNo ratings yet
- Diabetes Mellitus: Regulation of Blood GlucoseDocument65 pagesDiabetes Mellitus: Regulation of Blood GlucoseReggae BautistaNo ratings yet
- Osce ReviewerDocument119 pagesOsce Reviewerchiaruuh tNo ratings yet
- Presented By: V.Suhasini M-Pharm Department of PharmaceuticsDocument33 pagesPresented By: V.Suhasini M-Pharm Department of PharmaceuticstasniyanNo ratings yet
- Heinemann2014 PDFDocument9 pagesHeinemann2014 PDFRika Rahma PutriNo ratings yet
- Insulin Therapy A Pocket GuideDocument86 pagesInsulin Therapy A Pocket Guiderizkyfaraheigha89No ratings yet
- The Role of Prandial Insulin After Basal Optimization (Slide Intention)Document25 pagesThe Role of Prandial Insulin After Basal Optimization (Slide Intention)arisa_ebinaNo ratings yet
- Practical Guide To Insulin Therapy in Type 2 Diabetes: January 2011Document91 pagesPractical Guide To Insulin Therapy in Type 2 Diabetes: January 2011muhhasanalbolkiah saidNo ratings yet
- Practical Guide To Insulin TherapyDocument40 pagesPractical Guide To Insulin TherapyjeyakanthaNo ratings yet
- Intensive Insulin TherapyDocument54 pagesIntensive Insulin TherapynickhilraoNo ratings yet
- Diabetes MCQ 011215 PDFDocument6 pagesDiabetes MCQ 011215 PDFRawda Ibrahim100% (2)
- Guía NICe 2022Document55 pagesGuía NICe 2022Lucila BernasconiNo ratings yet
- Practical Guidance On The Use of Premix Insulin - FinalDocument14 pagesPractical Guidance On The Use of Premix Insulin - FinalJonesius Eden ManoppoNo ratings yet
- An Introduction To Insulin TherapyDocument23 pagesAn Introduction To Insulin TherapyOrion JohnNo ratings yet
- DCA-Coalition Insulin GuidelinesDocument5 pagesDCA-Coalition Insulin GuidelinesNabihah BarirNo ratings yet
- Meglitinide Analogues Are Classified As Insulin Secretagogues and Have Actions andDocument6 pagesMeglitinide Analogues Are Classified As Insulin Secretagogues and Have Actions andRifqoh Aulia AlthofunnisaNo ratings yet
- Insulin Treatment in DiabetesDocument86 pagesInsulin Treatment in DiabetesAhsan Rauf100% (1)
- Non-Critically Ill Hyperglycemia ManagementDocument39 pagesNon-Critically Ill Hyperglycemia ManagementHerry KongkoNo ratings yet
- Forum For Injection Technique Malaysia: Optimising Diabetes CareDocument64 pagesForum For Injection Technique Malaysia: Optimising Diabetes CareShaileene SheignNo ratings yet
- Diabetes and Pregnancy An Endocrine Society Clinical Practice Guideline ProvideDocument76 pagesDiabetes and Pregnancy An Endocrine Society Clinical Practice Guideline Providediabetes asiaNo ratings yet
- 121 1 Physicochemical Analytical Procedures For InsulinsDocument3 pages121 1 Physicochemical Analytical Procedures For InsulinssofianesedkaouiNo ratings yet
- CH 67Document14 pagesCH 67john mwangiNo ratings yet
- Diabetes Drug Notes (2022)Document393 pagesDiabetes Drug Notes (2022)evansNo ratings yet
- NovoRapid (Insulin Aspart) PDFDocument113 pagesNovoRapid (Insulin Aspart) PDFAchmad SuryadiNo ratings yet