You might also like
- Poisoning in ChildrenDocument46 pagesPoisoning in ChildrenPooja ChapdiNo ratings yet
- 2 AnticholinesterasesDocument55 pages2 AnticholinesterasesSudhakar LakavathNo ratings yet
- Organophosphate PoisoningDocument40 pagesOrganophosphate PoisoningMadhu Sudhan PandeyaNo ratings yet
- Toxicology in Critical Care: by Khairunnisa. Mansoor Instructor Acknowledgement: CCN TeamDocument28 pagesToxicology in Critical Care: by Khairunnisa. Mansoor Instructor Acknowledgement: CCN Teamshimama kanwalNo ratings yet
- Emergency Care For MO - General Approach To Poison ManagementDocument40 pagesEmergency Care For MO - General Approach To Poison Managementanupam mishraNo ratings yet
- Toxicology: PWM Olly Indrajani 2012Document57 pagesToxicology: PWM Olly Indrajani 2012arieska daraNo ratings yet
- Poisoning in ChildrenDocument46 pagesPoisoning in ChildrenpediatricsNo ratings yet
- Toxicology: PWM Olly Indrajani 2012Document54 pagesToxicology: PWM Olly Indrajani 2012Yuni IHNo ratings yet
- Acute Toxicity 2Document39 pagesAcute Toxicity 2Meraol HusseinNo ratings yet
- General Strategies For Management of Toxic EventsDocument78 pagesGeneral Strategies For Management of Toxic EventsMusa yohanaNo ratings yet
- Envenomation and IntoxicationDocument37 pagesEnvenomation and IntoxicationYoelBagusGiartoNo ratings yet
- Drug Overdose and PoisoningDocument64 pagesDrug Overdose and Poisoningsembakarani thevagumaranNo ratings yet
- Poisoning and ManagementDocument53 pagesPoisoning and ManagementYusuf Nawaz KhanNo ratings yet
- TOXICOLOGY (Shortened) (2021)Document66 pagesTOXICOLOGY (Shortened) (2021)Joel SaluNo ratings yet
- Pest ControlDocument76 pagesPest ControlHumraz KhanNo ratings yet
- Poisoning & BitesDocument12 pagesPoisoning & BitesJudy HandlyNo ratings yet
- Emergency 2Document86 pagesEmergency 2Harley Justiniani Dela CruzNo ratings yet
- PoisoningDocument36 pagesPoisoningsalah almozahemNo ratings yet
- Op and Oc Comp ToxiDocument37 pagesOp and Oc Comp ToxiSRINIVASAN GnanasabapathyNo ratings yet
- Problem 6 KGD: Maria Marcella 405090007Document121 pagesProblem 6 KGD: Maria Marcella 405090007Yessica TheresiaNo ratings yet
- Poisoning & Its ManagementDocument23 pagesPoisoning & Its ManagementdrugdrugNo ratings yet
- General Management of PoisoningDocument36 pagesGeneral Management of PoisoningKIPA SHRESTHANo ratings yet
- Poison Intro GaseousDocument73 pagesPoison Intro GaseouspikachuNo ratings yet
- Christiny P2 KGDDocument134 pagesChristiny P2 KGDrikarikaNo ratings yet
- PoisoningDocument89 pagesPoisoningrosana james100% (1)
- Poisoning II FinalDocument45 pagesPoisoning II FinalBi PinNo ratings yet
- A Patient of Poisoning in ICU (Ankit Jain)Document48 pagesA Patient of Poisoning in ICU (Ankit Jain)SharryNo ratings yet
- 71134lecture 6Document27 pages71134lecture 6azizNo ratings yet
- Toxicology Lect 2Document31 pagesToxicology Lect 2aneecaNo ratings yet
- Classification of PoisonsDocument73 pagesClassification of PoisonspikachuNo ratings yet
- Pediatric PoisoningDocument47 pagesPediatric PoisoningDr-Jagadeesh Mangamoori75% (4)
- PARAQUAT POISIONING 3rd Block Imed COMPLIEDDocument15 pagesPARAQUAT POISIONING 3rd Block Imed COMPLIEDMohil PratapNo ratings yet
- Cardiotoxicology ToxicologyDocument41 pagesCardiotoxicology ToxicologyIncha MaayaloNo ratings yet
- KGD 2 IvanDocument92 pagesKGD 2 IvanrikarikaNo ratings yet
- C1-Pediatrics 5th-Lec 1Document10 pagesC1-Pediatrics 5th-Lec 1عمر احمد شاكرNo ratings yet
- b7 PPT, AntihistaminesDocument56 pagesb7 PPT, AntihistaminesKeziah GillNo ratings yet
- Organophosphoruspoisoning 180211164511Document21 pagesOrganophosphoruspoisoning 180211164511Happy chifundaNo ratings yet
- Pesticide PoisoningDocument37 pagesPesticide PoisoningShorouk selimmNo ratings yet
- 14.4.20 Fn-PoisoningDocument43 pages14.4.20 Fn-PoisoninglisafelixNo ratings yet
- Chapter 34Document4 pagesChapter 34monster40lbsNo ratings yet
- Organo Phosphate Poisoning by DR Gireesh Kumar K PDocument16 pagesOrgano Phosphate Poisoning by DR Gireesh Kumar K PAETCM Emergency medicineNo ratings yet
- Poisoning in Children: Ramin Nazari, MD March 2015Document187 pagesPoisoning in Children: Ramin Nazari, MD March 2015jennifer sampangNo ratings yet
- Kerosene Toxicity - 1657101641Document22 pagesKerosene Toxicity - 1657101641Mohil PratapNo ratings yet
- Salicylate Poisoning DR Moses KazevuDocument25 pagesSalicylate Poisoning DR Moses KazevuMoses Jr KazevuNo ratings yet
- Paraquat PoisoningDocument45 pagesParaquat PoisoningM. O. PHC HOLAVANAHALLYNo ratings yet
- Malignant HyperthermiaDocument57 pagesMalignant HyperthermiaSuvadeep SenNo ratings yet
- 33-36 Medications PDFDocument15 pages33-36 Medications PDFJeraldine GumpalNo ratings yet
- General Measure in The Management of PoisoningDocument43 pagesGeneral Measure in The Management of PoisoningCharlotte Anne Villero TiuNo ratings yet
- POISONING EmsDocument16 pagesPOISONING EmsJames AbendanNo ratings yet
- Pharma Review FinalsDocument31 pagesPharma Review FinalsLanz Andrei MatociñosNo ratings yet
- Organophosphates and Carbamates PoisoningDocument34 pagesOrganophosphates and Carbamates PoisoningMuhammad Hammad Maahi100% (1)
- Classification: 1. Natural AlkaloidsDocument14 pagesClassification: 1. Natural AlkaloidsManikanta GupthaNo ratings yet
- Poisoning: Presented By: Ivan AvenadoDocument11 pagesPoisoning: Presented By: Ivan AvenadoIvan Liquiran Avenado0% (1)
- PoisoningDocument52 pagesPoisoninganimesh pandaNo ratings yet
- Corosive PoisoningDocument16 pagesCorosive Poisoninglitan dasNo ratings yet
- Paraquat PoisoningDocument12 pagesParaquat PoisoningJean LlausasNo ratings yet
- The Biochemical Pathway of Paraquat ToxicityDocument16 pagesThe Biochemical Pathway of Paraquat ToxicitysuderiNo ratings yet
- Acute Poisoning in Adults: Dr. S.P. Hewawasam MBBS, MDDocument76 pagesAcute Poisoning in Adults: Dr. S.P. Hewawasam MBBS, MDSamapriya Pasan Hewawasam100% (1)
- Comparison of Autocorrelation Between CV-RISK Independent Variables in Groups With and Without History of Cardiovascular DiseasesDocument9 pagesComparison of Autocorrelation Between CV-RISK Independent Variables in Groups With and Without History of Cardiovascular DiseasesYohanes FirmansyahNo ratings yet
- Non-Powder Lateral Penetrating CraniocerebralDocument14 pagesNon-Powder Lateral Penetrating CraniocerebralYohanes FirmansyahNo ratings yet
- The Role of The WTO in Mediate Dispute Palm Oil Between Indonesia and The European UnionDocument18 pagesThe Role of The WTO in Mediate Dispute Palm Oil Between Indonesia and The European UnionYohanes FirmansyahNo ratings yet
- Uji Antibakteri Dan Antijamur V-Cleanser Foam Dari Bahan Baku Daun Sirih (Piper Betle L.)Document4 pagesUji Antibakteri Dan Antijamur V-Cleanser Foam Dari Bahan Baku Daun Sirih (Piper Betle L.)Yohanes FirmansyahNo ratings yet
- Kemampuan Klinis Neutrophil Lymphocyte Ratio (NLR) Pada Kehamilan Sebagai Prediktor PreeklamsiaDocument9 pagesKemampuan Klinis Neutrophil Lymphocyte Ratio (NLR) Pada Kehamilan Sebagai Prediktor PreeklamsiaYohanes FirmansyahNo ratings yet
- Skin Manifestation in CovidDocument8 pagesSkin Manifestation in CovidWinniaTanelyNo ratings yet
- Strategy Within Limitations During COVID-19 Pandemic in IndonesiaDocument3 pagesStrategy Within Limitations During COVID-19 Pandemic in IndonesiaYohanes FirmansyahNo ratings yet
- New Approach To Deep Diabetic Foot Ulcer (DFU) Treatment-Potential of Secretome From Wharton's Jelly Mesenchymal Stem Cell TherapyDocument6 pagesNew Approach To Deep Diabetic Foot Ulcer (DFU) Treatment-Potential of Secretome From Wharton's Jelly Mesenchymal Stem Cell TherapyYohanes FirmansyahNo ratings yet
- Morpot 23-26 Feb 2018Document92 pagesMorpot 23-26 Feb 2018Yohanes FirmansyahNo ratings yet
- The Adjustment of Neurosurgery Practices During COVID-19Document5 pagesThe Adjustment of Neurosurgery Practices During COVID-19Yohanes FirmansyahNo ratings yet
- Implementation of International Relations On Illegal Fishing Activities by Chinese Fisherman in The Exclusive Economic Zone of The Republic of Indonesia Natural IslandDocument14 pagesImplementation of International Relations On Illegal Fishing Activities by Chinese Fisherman in The Exclusive Economic Zone of The Republic of Indonesia Natural IslandYohanes FirmansyahNo ratings yet
- 1 New Approachment of Creeping Eruption ManagementDocument5 pages1 New Approachment of Creeping Eruption ManagementannibaNo ratings yet
- Two Side Coins of Euthanasia Mercy-Killing or Evil According To Human Rights, Religion, Ethics and The LawDocument8 pagesTwo Side Coins of Euthanasia Mercy-Killing or Evil According To Human Rights, Religion, Ethics and The LawYohanes FirmansyahNo ratings yet
- Neutrophils-Lymphocytes Ratio (NLR) and Platelet-Lymphocytes Ratio (PLR) As Predictors of NSTEMI EventDocument9 pagesNeutrophils-Lymphocytes Ratio (NLR) and Platelet-Lymphocytes Ratio (PLR) As Predictors of NSTEMI EventYohanes FirmansyahNo ratings yet
- New Approach To Skin Burn Treatment Potential of Secretome From Wharton's Jelly Mesenchymal Stem Cell TherapyDocument6 pagesNew Approach To Skin Burn Treatment Potential of Secretome From Wharton's Jelly Mesenchymal Stem Cell TherapyYohanes FirmansyahNo ratings yet
- Neurotropic Ulcer On Morbus Hansen MultibacillaryDocument3 pagesNeurotropic Ulcer On Morbus Hansen MultibacillaryYohanes FirmansyahNo ratings yet
- Improvement of Random Blood Glucose On Diabetes Mellitus Type II Patients With Medication Box Interventions and Individual Education MethodsDocument6 pagesImprovement of Random Blood Glucose On Diabetes Mellitus Type II Patients With Medication Box Interventions and Individual Education MethodsYohanes FirmansyahNo ratings yet
- A Law Perspective The Thin Curtain Between Malpractice and Medical RiskDocument7 pagesA Law Perspective The Thin Curtain Between Malpractice and Medical RiskYohanes FirmansyahNo ratings yet
- KappaDocument6 pagesKappaYohanes FirmansyahNo ratings yet
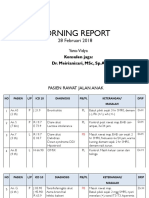
- Morning Report 28-02-18Document37 pagesMorning Report 28-02-18Yohanes FirmansyahNo ratings yet
- Morning Report9-12 Maret 2018Document107 pagesMorning Report9-12 Maret 2018Yohanes FirmansyahNo ratings yet
- Final Pit 2020 IsbnDocument20 pagesFinal Pit 2020 IsbnYohanes FirmansyahNo ratings yet
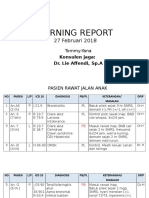
- Morning Report 27-02-18Document39 pagesMorning Report 27-02-18Yohanes FirmansyahNo ratings yet
- Morning Report: 9 Februari 2018Document20 pagesMorning Report: 9 Februari 2018Yohanes FirmansyahNo ratings yet
- Morning Report: 9 Februari 2018Document20 pagesMorning Report: 9 Februari 2018Yohanes FirmansyahNo ratings yet
- Morning Report 23-01-18Document36 pagesMorning Report 23-01-18Yohanes FirmansyahNo ratings yet
- Morning Report 11-3-2018Document23 pagesMorning Report 11-3-2018Yohanes FirmansyahNo ratings yet
- Morning Report 20-1-2018Document20 pagesMorning Report 20-1-2018Yohanes FirmansyahNo ratings yet
- Morning Report 13-02-2018Document20 pagesMorning Report 13-02-2018Yohanes FirmansyahNo ratings yet
- Morning Report 11-2-2018Document21 pagesMorning Report 11-2-2018Yohanes FirmansyahNo ratings yet
- T10 - PointersDocument3 pagesT10 - PointersGlory of Billy's Empire Jorton KnightNo ratings yet
- BDRRM Sample Draft EoDocument5 pagesBDRRM Sample Draft EoJezreelJhizelRamosMendozaNo ratings yet
- Tugas Inggris Text - Kelas 9Document27 pagesTugas Inggris Text - Kelas 9salviane.theandra.jNo ratings yet
- Shades Eq Gloss Large Shade ChartDocument2 pagesShades Eq Gloss Large Shade ChartmeganNo ratings yet
- Chapter 12Document15 pagesChapter 12kk5522No ratings yet
- Whitepaper ITES Industry PotentialDocument6 pagesWhitepaper ITES Industry PotentialsamuraiharryNo ratings yet
- Fish Culture in Ponds: Extension Bulletin No. 103Document32 pagesFish Culture in Ponds: Extension Bulletin No. 103Bagas IndiantoNo ratings yet
- Module 4 How To Make Self-Rescue Evacuation Maps?Document85 pagesModule 4 How To Make Self-Rescue Evacuation Maps?RejieNo ratings yet
- Merchant Shipping MINIMUM SAFE MANNING Regulations 2016Document14 pagesMerchant Shipping MINIMUM SAFE MANNING Regulations 2016Arthur SchoutNo ratings yet
- DISTRICT CENSUS HANDBOOK North GoaDocument190 pagesDISTRICT CENSUS HANDBOOK North Goants1020No ratings yet
- Old Highland Park Baptist Church E01Document74 pagesOld Highland Park Baptist Church E01Lawrence Garner100% (2)
- Travelstart Ticket (ZA10477979) PDFDocument2 pagesTravelstart Ticket (ZA10477979) PDFMatthew PretoriusNo ratings yet
- Beer Lambert'S Law: Dr. Swastika Das Professor of ChemistryDocument19 pagesBeer Lambert'S Law: Dr. Swastika Das Professor of ChemistryShabanaNo ratings yet
- Daily Plankton Agrabinta CianjurDocument141 pagesDaily Plankton Agrabinta CianjurPutra Cahya GemilangNo ratings yet
- Advanced Statistical Approaches To Quality: INSE 6220 - Week 4Document44 pagesAdvanced Statistical Approaches To Quality: INSE 6220 - Week 4picalaNo ratings yet
- Lupon National Comprehensive High School Ilangay, Lupon, Davao Oriental Grade 10-Household ServicesDocument4 pagesLupon National Comprehensive High School Ilangay, Lupon, Davao Oriental Grade 10-Household ServicesJohn Eirhene Intia BarreteNo ratings yet
- Computer in Community Pharmacy by Adnan Sarwar ChaudharyDocument10 pagesComputer in Community Pharmacy by Adnan Sarwar ChaudharyDr-Adnan Sarwar Chaudhary100% (1)
- De On Tap So 4-6Document8 pagesDe On Tap So 4-6Quy DoNo ratings yet
- Saes T 883Document13 pagesSaes T 883luke luckyNo ratings yet
- Lyka Kendall B. Adres: Personal Na ImpormasyonDocument2 pagesLyka Kendall B. Adres: Personal Na ImpormasyonKendall BarbietoNo ratings yet
- IBS and SIBO Differential Diagnosis, SiebeckerDocument1 pageIBS and SIBO Differential Diagnosis, SiebeckerKrishna DasNo ratings yet
- Wits Appraisalnof Jaw Disharmony by JOHNSONDocument20 pagesWits Appraisalnof Jaw Disharmony by JOHNSONDrKamran MominNo ratings yet
- Acronyms and AbbreviationsDocument875 pagesAcronyms and AbbreviationsLacky KrishnanNo ratings yet
- Menara PMB Assessment Criteria Score SummaryDocument2 pagesMenara PMB Assessment Criteria Score SummarySyerifaizal Hj. MustaphaNo ratings yet
- CCNP SWITCH 300-115 - Outline of The Official Study GuideDocument31 pagesCCNP SWITCH 300-115 - Outline of The Official Study GuidehammiesinkNo ratings yet
- Vignyapan 18-04-2024Document16 pagesVignyapan 18-04-2024adil1787No ratings yet
- 3 A Sanitary Standards Quick Reference GuideDocument98 pages3 A Sanitary Standards Quick Reference GuideLorettaMayNo ratings yet
- Polyembryony &its ImportanceDocument17 pagesPolyembryony &its ImportanceSURIYA PRAKASH GNo ratings yet
- Capital Structure and Leverage: Multiple Choice: ConceptualDocument53 pagesCapital Structure and Leverage: Multiple Choice: ConceptualArya StarkNo ratings yet
- SLTMobitel AssignmentDocument3 pagesSLTMobitel AssignmentSupun ChandrakanthaNo ratings yet