You might also like
- Concise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryFrom EverandConcise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryNo ratings yet
- Leukemia Treatment Regimens 7937Document3 pagesLeukemia Treatment Regimens 7937Irfan FathurrahmanNo ratings yet
- A Statistical Inquiry Into the Nature and Treatment of EpilepsyFrom EverandA Statistical Inquiry Into the Nature and Treatment of EpilepsyNo ratings yet
- Management of Malaria in Children: Update 2008: GuidelinesDocument5 pagesManagement of Malaria in Children: Update 2008: GuidelinesSaumilNo ratings yet
- Pituitary Tumors: A Clinical CasebookFrom EverandPituitary Tumors: A Clinical CasebookLisa B. NachtigallNo ratings yet
- Tuberculosis Treatment, MDR, XDR, Resistance, Prophylaxis, VaccinationDocument44 pagesTuberculosis Treatment, MDR, XDR, Resistance, Prophylaxis, Vaccinationskeisham11No ratings yet
- Recent TB Treatment GuidelinesDocument28 pagesRecent TB Treatment GuidelinesDr venkatesh jalluNo ratings yet
- Central Nervous System InfectionsDocument9 pagesCentral Nervous System InfectionsSaddamNo ratings yet
- Antiparasitic Agents RevisedDocument94 pagesAntiparasitic Agents RevisedJe SantosNo ratings yet
- Malaria: Public Health Division, Directorate of Health Services Thiruvananthapuram June 2016Document15 pagesMalaria: Public Health Division, Directorate of Health Services Thiruvananthapuram June 2016Ajan MjNo ratings yet
- Azithromycin NMFv1.0 Full 20180620Document5 pagesAzithromycin NMFv1.0 Full 20180620Lütfiye ÖzlemNo ratings yet
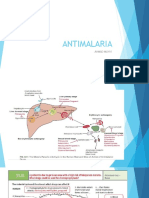
- ANTIMALARIADocument15 pagesANTIMALARIABunga Tresna MaduriNo ratings yet
- National Malaria Drug PolicyDocument22 pagesNational Malaria Drug Policydocsaurabh777No ratings yet
- Antibiotic Guidelines For PediatricsDocument33 pagesAntibiotic Guidelines For PediatricsVarshini Tamil SelvanNo ratings yet
- Outline of Presentation: Evolving Malaria Control Strategies in India. NVBDCPDocument33 pagesOutline of Presentation: Evolving Malaria Control Strategies in India. NVBDCPritikaritikaNo ratings yet
- Guidance On The Rational Use of RH Kit 3 (Post Rape Management)Document8 pagesGuidance On The Rational Use of RH Kit 3 (Post Rape Management)hiba.khellowNo ratings yet
- Anti MalariaDocument49 pagesAnti MalariaYIKI ISAACNo ratings yet
- Rntcp-Revised National Tuberculosis Control ProgrammeDocument29 pagesRntcp-Revised National Tuberculosis Control ProgrammedranshulitrivediNo ratings yet
- Intensified Tuberculosis MeningitisDocument18 pagesIntensified Tuberculosis MeningitisGina ArianiNo ratings yet
- Azithromycin Monograph - PaediatricDocument7 pagesAzithromycin Monograph - PaediatrictynNo ratings yet
- National Maria Drug Policy 2007Document12 pagesNational Maria Drug Policy 2007drbeerappa janpetNo ratings yet
- Oxaciline PDFDocument7 pagesOxaciline PDFamatoryfictionliteraNo ratings yet
- VVC Vulvo VaginalDocument2 pagesVVC Vulvo VaginalVshn VardhnNo ratings yet
- 1.CD Control Program: RD RDDocument18 pages1.CD Control Program: RD RDKen Mark CatubigNo ratings yet
- TB PosterDocument1 pageTB PosterSucie 1997No ratings yet
- Adverse Effects of Anti Tubercular Drugs. MDR TBDocument75 pagesAdverse Effects of Anti Tubercular Drugs. MDR TBDr.U.P.Rathnakar.MD.DIH.PGDHM100% (1)
- Antimicrobial Therapy in Sepsis PDFDocument38 pagesAntimicrobial Therapy in Sepsis PDFTatik HandayaniNo ratings yet
- Ovarian Cancer Treatment Regimens - Print Article - Cancer Therapy AdvisorDocument5 pagesOvarian Cancer Treatment Regimens - Print Article - Cancer Therapy AdvisorAnonymous g1hIPZNo ratings yet
- Peptic Ulcer Disease DrugsDocument6 pagesPeptic Ulcer Disease DrugsApple MaeNo ratings yet
- Trastuzumab (Intravenous) Including Biosimilars of Trastuzumab - Drug Information - UpToDateDocument20 pagesTrastuzumab (Intravenous) Including Biosimilars of Trastuzumab - Drug Information - UpToDateDenys Romero100% (1)
- College of Nursing: Drug Study PharmacologyDocument1 pageCollege of Nursing: Drug Study PharmacologyPoinsithia OrlandaNo ratings yet
- Targocid Article 30 Referral Annex III - enDocument32 pagesTargocid Article 30 Referral Annex III - enDR JAMAL WARISNo ratings yet
- Uterine Sarcoma - Pharmacologic Management - Cancer Therapy AdvisorDocument32 pagesUterine Sarcoma - Pharmacologic Management - Cancer Therapy AdvisorIrfan FathurrahmanNo ratings yet
- LYRICE ProtocolDocument6 pagesLYRICE ProtocolInas UthmanNo ratings yet
- Princy N. Kumar, MDDocument8 pagesPrincy N. Kumar, MDfeedodeedoNo ratings yet
- Pustaka AHFS - ESODocument8 pagesPustaka AHFS - ESORindang RizkyNo ratings yet
- Antimycobacterial Drug StudyDocument5 pagesAntimycobacterial Drug StudyKathNo ratings yet
- Management of MalariaDocument55 pagesManagement of MalariaAnu SinhaNo ratings yet
- K25. Malaria Pada AnakDocument39 pagesK25. Malaria Pada AnakayapillaiNo ratings yet
- Endometrialcarcinoma r0416 7941Document2 pagesEndometrialcarcinoma r0416 7941crisibarra911No ratings yet
- Malaria Control Program (Hard Copy)Document10 pagesMalaria Control Program (Hard Copy)JacqColumnaNo ratings yet
- Sepsis and Catheter Infections: Early Conversion From IV To Oral AntibioticsDocument4 pagesSepsis and Catheter Infections: Early Conversion From IV To Oral AntibioticsChaim HerreraNo ratings yet
- Tatalaksana Malaria Pada AnakDocument41 pagesTatalaksana Malaria Pada AnakJoanNo ratings yet
- Azithromycin Medication PDFDocument1 pageAzithromycin Medication PDFmp1757No ratings yet
- Vaccinations Guideline Summary 2022Document4 pagesVaccinations Guideline Summary 2022Faisal PNo ratings yet
- Slide Malaria Prevention TimikaDocument45 pagesSlide Malaria Prevention Timikastivana26No ratings yet
- Kanamycin (Mode of Administration)Document3 pagesKanamycin (Mode of Administration)Waseem MaroofiNo ratings yet
- Malaria Dalam Kehamilan: Erni Juwita Nelwan Divisi Tropik Dan Penyakit Infeksi Fkui - RSCMDocument27 pagesMalaria Dalam Kehamilan: Erni Juwita Nelwan Divisi Tropik Dan Penyakit Infeksi Fkui - RSCMadrianamarshaNo ratings yet
- Pumonary Tuberculosis in Pregnancy PALLAVIDocument42 pagesPumonary Tuberculosis in Pregnancy PALLAVIJyothsna DeepNo ratings yet
- Daepoch Protocolo BccancerDocument9 pagesDaepoch Protocolo BccancerLuiz MeloNo ratings yet
- Role of ACT, S & WHO Guidlines For The Treatment of MalariaDocument34 pagesRole of ACT, S & WHO Guidlines For The Treatment of MalariasalmanNo ratings yet
- Treatment of TB in Adults: by Dr. Irfhan Ali Hyder AliDocument45 pagesTreatment of TB in Adults: by Dr. Irfhan Ali Hyder AliInspireGutsNo ratings yet
- Enteral InfectionsDocument6 pagesEnteral InfectionsAshley CheungNo ratings yet
- Guideline: Antibiotic Drug Monitoring: Aminoglycosides and GlycopeptidesDocument8 pagesGuideline: Antibiotic Drug Monitoring: Aminoglycosides and GlycopeptidesKenRodulfReyesVillaruelNo ratings yet
- Nica Chua - Hospital Pharmacy Internship Daily Activity Report-Day 33 MajorDocument5 pagesNica Chua - Hospital Pharmacy Internship Daily Activity Report-Day 33 MajorMa Victoria ChuaNo ratings yet
- Malaria Prevention TimikaDocument41 pagesMalaria Prevention Timikastivana26No ratings yet
- Treatment Update For Scrub Typhus: ReviewDocument5 pagesTreatment Update For Scrub Typhus: ReviewSandeep SoniNo ratings yet
- Revision 1Document21 pagesRevision 1NaifmxNo ratings yet
- I.5 - Ab Necrotizing FasciitisDocument16 pagesI.5 - Ab Necrotizing FasciitisShameen KhanNo ratings yet
- A Knowledge, (KAP) : Study Dengue Among KangsarDocument7 pagesA Knowledge, (KAP) : Study Dengue Among Kangsarsyuhaida deqsuNo ratings yet
- Swaddiwudhipong (1992)Document5 pagesSwaddiwudhipong (1992)syuhaida deqsuNo ratings yet
- Dear MR Kilmer Chapter 7Document7 pagesDear MR Kilmer Chapter 7syuhaida deqsuNo ratings yet
- Questions On Archimedes PrincipleDocument2 pagesQuestions On Archimedes Principlesyuhaida deqsuNo ratings yet
- Hand Foot MouthDocument6 pagesHand Foot MouthbinbinadiNo ratings yet
- DC TyphusDocument18 pagesDC Typhussyuhaida deqsuNo ratings yet
- Questions On Archimedes PrincipleDocument2 pagesQuestions On Archimedes Principlesyuhaida deqsuNo ratings yet
- Msds Caustic 50 TDC 2010Document6 pagesMsds Caustic 50 TDC 2010syuhaida deqsuNo ratings yet
- DC TyphusDocument18 pagesDC Typhussyuhaida deqsuNo ratings yet
- Smear Negative TBDocument53 pagesSmear Negative TBsyuhaida deqsuNo ratings yet
- ORTHOSIS - and ProthesisDocument112 pagesORTHOSIS - and Prothesismanjukumard2007100% (1)
- Benefits of TED TalkslDocument1 pageBenefits of TED TalkslPahlawan HalusinasiNo ratings yet
- Hospital FinalDocument82 pagesHospital FinalEzedin KedirNo ratings yet
- Haemodialysis Quality StandardsDocument59 pagesHaemodialysis Quality StandardsshawkishahrhNo ratings yet
- Decision Making Pain Ramamurthy PDFDocument319 pagesDecision Making Pain Ramamurthy PDFDian wNo ratings yet
- Biomechanics of The HipDocument12 pagesBiomechanics of The HipSimon Ocares AranguizNo ratings yet
- NICU ReportDocument7 pagesNICU ReportoapsdoaksdokaNo ratings yet
- Pacemakers and Implantable Cardioverter DefibrillatorsDocument10 pagesPacemakers and Implantable Cardioverter Defibrillatorsnoorhadi.n10No ratings yet
- Prema V Opalustre MIHDocument8 pagesPrema V Opalustre MIHbrigidgaffneyNo ratings yet
- Photo Therapy and Bili LightDocument5 pagesPhoto Therapy and Bili LightLyra LorcaNo ratings yet
- Study Protocol (Study Plan)Document19 pagesStudy Protocol (Study Plan)Deana NamirembeNo ratings yet
- Anavar StackDocument3 pagesAnavar Stackbond99999No ratings yet
- Abg CaseAnswersDocument7 pagesAbg CaseAnswersDiana HyltonNo ratings yet
- Dystocia: Presenter-Dr Aakriti Bhandari Moderated By-Dr. Ashok KumarDocument60 pagesDystocia: Presenter-Dr Aakriti Bhandari Moderated By-Dr. Ashok KumarAvishkar AgrawalNo ratings yet
- Maxillary Sinus Surgery PDFDocument17 pagesMaxillary Sinus Surgery PDFHossam Elden Helmy HaridyNo ratings yet
- Nurse AnesthesiaDocument3 pagesNurse Anesthesiaapi-348841675No ratings yet
- NIAC Hospital Network List PPN and NON PPNDocument3,464 pagesNIAC Hospital Network List PPN and NON PPNluckynaveenrajNo ratings yet
- Pediatric Movement DisordersDocument15 pagesPediatric Movement DisordersMia FernandezNo ratings yet
- Pai 1Document6 pagesPai 1arieq bustamanNo ratings yet
- Chapter 1 Overview of Critical Care StudentDocument40 pagesChapter 1 Overview of Critical Care StudentEmilyNo ratings yet
- Autism Spectrum DisorderDocument13 pagesAutism Spectrum Disorderapi-283801172No ratings yet
- Kronenberg Williams Textbook of Endocrinology, 11th EdDocument3 pagesKronenberg Williams Textbook of Endocrinology, 11th EdRahim4411No ratings yet
- Aubrey PalermoDocument4 pagesAubrey PalermoFOX42 NewsNo ratings yet
- Biology 453 - Comparative Vert. Anatomy WEEK 1, LAB 1: Anatomical Terms & Introduction To Chordates AssignmentsDocument10 pagesBiology 453 - Comparative Vert. Anatomy WEEK 1, LAB 1: Anatomical Terms & Introduction To Chordates AssignmentsKerbie Jayd0% (1)
- Radiography of STN and AbdomenDocument18 pagesRadiography of STN and AbdomenSudil PaudyalNo ratings yet
- Duo Service ManualDocument108 pagesDuo Service ManualDanniel SchaafNo ratings yet
- Apollo Gleneagles Hospitals: The Next Steps For GrowthDocument16 pagesApollo Gleneagles Hospitals: The Next Steps For Growthyashi mittalNo ratings yet
- Hydrocephalus: Mr. Fadi J. Zaben RN MSN IMET2000, Ramallah February, 2013Document30 pagesHydrocephalus: Mr. Fadi J. Zaben RN MSN IMET2000, Ramallah February, 2013WisnuBaskoro100% (1)
- Healing The Father Wound: A 40 Year JourneyDocument8 pagesHealing The Father Wound: A 40 Year JourneyJed Diamond100% (1)
- Chison Ivis 60 Expert PDFDocument3 pagesChison Ivis 60 Expert PDFHAITHAMNo ratings yet