You might also like
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Configuration Steps - Settlement Management in S - 4 HANA - SAP Blogs PDFDocument34 pagesConfiguration Steps - Settlement Management in S - 4 HANA - SAP Blogs PDFKiran KagitapuNo ratings yet
- Measuring Downstream Supply Chain Performance in the Oil IndustryDocument86 pagesMeasuring Downstream Supply Chain Performance in the Oil IndustryKiran KagitapuNo ratings yet
- Enhancements - Sales Order VA01 - VA02 - VA03 - My Experiments With ABAP PDFDocument7 pagesEnhancements - Sales Order VA01 - VA02 - VA03 - My Experiments With ABAP PDFKiran KagitapuNo ratings yet
- Transaction: SE38 Then Enter Program "ZOTC - PR - R - YHPP - COND - CREATE"Document2 pagesTransaction: SE38 Then Enter Program "ZOTC - PR - R - YHPP - COND - CREATE"Kiran KagitapuNo ratings yet
- Setting Up Purchase Order Release Strategy - SAP BlogsDocument21 pagesSetting Up Purchase Order Release Strategy - SAP BlogsKiran KagitapuNo ratings yet
- ArchievingDocument92 pagesArchievingKiran KagitapuNo ratings yet
- Rebate Process in SAP SDDocument5 pagesRebate Process in SAP SDKiran KagitapuNo ratings yet
- Rebate Process in SAP SDDocument5 pagesRebate Process in SAP SDKiran KagitapuNo ratings yet
- Configuration Steps - Settlement Management in S - 4 HANA - SAP Blogs PDFDocument34 pagesConfiguration Steps - Settlement Management in S - 4 HANA - SAP Blogs PDFKiran KagitapuNo ratings yet
- BP Stats Review 2018 Full ReportDocument56 pagesBP Stats Review 2018 Full ReportLorena DominguezNo ratings yet
- 1105ed68 5431previewDocument1 page1105ed68 5431previewKiran KagitapuNo ratings yet
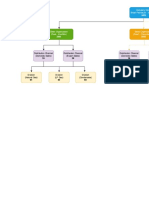
- Company Code Structure for Pearl Petroleum Sales and DistributionDocument2 pagesCompany Code Structure for Pearl Petroleum Sales and DistributionKiran KagitapuNo ratings yet
- Distribution Channel (Domestic Sales) Distribution Channel (Export Sales) Distribution Channel (Domestic Sales)Document2 pagesDistribution Channel (Domestic Sales) Distribution Channel (Export Sales) Distribution Channel (Domestic Sales)Kiran KagitapuNo ratings yet
- Untitled DiagramDocument2 pagesUntitled DiagramKiran KagitapuNo ratings yet
- Synthesis For PipelinesDocument2 pagesSynthesis For PipelinesKiran KagitapuNo ratings yet
- Sales statistics report by company code and addressDocument6 pagesSales statistics report by company code and addressKiran KagitapuNo ratings yet
- Dip Profiles DocumentationDocument89 pagesDip Profiles Documentationmurali83% (6)
- TSW ArchitectureDocument6 pagesTSW ArchitectureKiran KagitapuNo ratings yet
- Who Gets What From Imported Oil 2018Document4 pagesWho Gets What From Imported Oil 2018Kiran KagitapuNo ratings yet
- Work Allowance Claim FormDocument4 pagesWork Allowance Claim FormKiran KagitapuNo ratings yet
- Oil & Gas: June 2018Document41 pagesOil & Gas: June 2018Kiran KagitapuNo ratings yet
- Who Gets What From Imported Oil 2018Document4 pagesWho Gets What From Imported Oil 2018Kiran KagitapuNo ratings yet
- Material Master DocumentsDocument23 pagesMaterial Master DocumentsKiran Kagitapu100% (1)
- BP Stats Review 2018 Oil SlidepackDocument11 pagesBP Stats Review 2018 Oil SlidepackKiran KagitapuNo ratings yet
- Define PlantsDocument2 pagesDefine PlantsKiran KagitapuNo ratings yet
- Card StatementDocument1 pageCard StatementKiran KagitapuNo ratings yet
- Oij Nom Detail01 DDocument54 pagesOij Nom Detail01 DKiran KagitapuNo ratings yet
- RAIL Subitems KiranDocument4 pagesRAIL Subitems KiranKiran KagitapuNo ratings yet
- Botswana Jde MappingDocument7 pagesBotswana Jde MappingKiran KagitapuNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 2012 Sedative Hypnotic DrugsDocument38 pages2012 Sedative Hypnotic DrugsHiwa Khidhir saaedNo ratings yet
- Lesson Plan - DrugsDocument5 pagesLesson Plan - Drugsapi-231745681100% (1)
- LECTURE 3 - Pharmacology of VasoconstrictorsDocument27 pagesLECTURE 3 - Pharmacology of VasoconstrictorsKIH 20162017No ratings yet
- 8B - Antianginal DrugsDocument70 pages8B - Antianginal Drugslalitrajindolia100% (1)
- Drug Study - IBRANCEDocument3 pagesDrug Study - IBRANCEKian HerreraNo ratings yet
- Attapulgite Vs CiproDocument6 pagesAttapulgite Vs CiproAyu Syifa NaufaliaNo ratings yet
- Davis-Oparil2018Document17 pagesDavis-Oparil2018neeraj glaNo ratings yet
- Daftar FormulariumDocument67 pagesDaftar FormulariumNandea Zulfana HendrawanNo ratings yet
- FDCs Banned 7 SEP 2018 - ListDocument9 pagesFDCs Banned 7 SEP 2018 - ListParthMairNo ratings yet
- Drug Study - DelanDocument3 pagesDrug Study - DelanJuliana Sophia DelanNo ratings yet
- MD Tanjil 22Document1 pageMD Tanjil 22wasi Wasikhan890yahoo.comNo ratings yet
- Zopiclone Report Sep09Document21 pagesZopiclone Report Sep09Iona KalosNo ratings yet
- Everything You Need to Know About StimulantsDocument4 pagesEverything You Need to Know About StimulantsLinh-Trang NguyenNo ratings yet
- Parada Murcchana & Rasa Kalpas - Kharliya & ParpatiDocument45 pagesParada Murcchana & Rasa Kalpas - Kharliya & ParpatiDimpal Zambare86% (7)
- Free Drug Bank GUIDE 1 PDFDocument76 pagesFree Drug Bank GUIDE 1 PDFRaouf Ra'fat Soliman100% (11)
- DoxycyclineDocument2 pagesDoxycyclinesleep whatNo ratings yet
- Ati RN Pharmacology Exam 2020 Latest Questions and AnswersDocument14 pagesAti RN Pharmacology Exam 2020 Latest Questions and AnswersPeggy Gebhart100% (35)
- Idsa Amr Guidance v3.0Document174 pagesIdsa Amr Guidance v3.0Sejla KotoricNo ratings yet
- Nasal Spray Condensed - HOW TO MAKE NASAL SPRAY FOR DRVGSDocument3 pagesNasal Spray Condensed - HOW TO MAKE NASAL SPRAY FOR DRVGSInés Grande BarrasNo ratings yet
- Ich - GCP Consolidated GuidelinesDocument22 pagesIch - GCP Consolidated Guidelinesapi-3709098No ratings yet
- Drug Calculations Reviewer For NursesDocument38 pagesDrug Calculations Reviewer For Nurseslia pescaderaNo ratings yet
- Glaxo SmithlineDocument3 pagesGlaxo SmithlinebhuvaneshkmrsNo ratings yet
- PT - Dayaanugerah Dewatasakti Jl. Taman Jemursari Selatan 1/ 7 Surabaya Nama Produck HNA Hna+Ppn Nama Produck HNA Hna+PpnDocument16 pagesPT - Dayaanugerah Dewatasakti Jl. Taman Jemursari Selatan 1/ 7 Surabaya Nama Produck HNA Hna+Ppn Nama Produck HNA Hna+PpnYuliSetiyantoNo ratings yet
- Ropivacaine Vs Bupivacaine PDFDocument6 pagesRopivacaine Vs Bupivacaine PDFJessica LawrenceNo ratings yet
- HS140 Unit 6 Quiz Study GuideDocument9 pagesHS140 Unit 6 Quiz Study GuideCrystal MendiolaNo ratings yet
- Drug Safety ReviewsDocument5 pagesDrug Safety ReviewsToronto StarNo ratings yet
- Preparation #: Paracetamol Tablets I. Objectives:: Pharmaceutical Dosage Forms Laboratory ManualDocument2 pagesPreparation #: Paracetamol Tablets I. Objectives:: Pharmaceutical Dosage Forms Laboratory Manuallalag yanNo ratings yet
- Daftar Sediaan Obat Nama Obat Obat Yang Dipakai Sediaan: Ratama AMADocument4 pagesDaftar Sediaan Obat Nama Obat Obat Yang Dipakai Sediaan: Ratama AMAtikaNo ratings yet
- Scnausea Protocol 1mar2012Document6 pagesScnausea Protocol 1mar2012Afra FitrianitaNo ratings yet
- Herb Drug InteractionsDocument15 pagesHerb Drug InteractionsdivakarmcNo ratings yet