You might also like
- Gastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandGastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- URINARY TRACT INFECTION CAUSES AND TREATMENTDocument6 pagesURINARY TRACT INFECTION CAUSES AND TREATMENTLourdes Fernandez CabreraNo ratings yet
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Diabetes MellitusDocument17 pagesDiabetes MellitusRuqayya KobatteNo ratings yet
- Providing Comfort During LaborDocument11 pagesProviding Comfort During LaborAndrea Marie SevillaNo ratings yet
- Threatened Abortion: Causes, Symptoms and TreatmentDocument9 pagesThreatened Abortion: Causes, Symptoms and TreatmentYien-yin MuachNo ratings yet
- 8. Care of Child With GI Dysfunction (1) ءءءءDocument44 pages8. Care of Child With GI Dysfunction (1) ءءءءNuhaNo ratings yet
- CAD - EBM September 2020 EditionDocument17 pagesCAD - EBM September 2020 EditionNaga Venkatamanoj Kumar PakalapatiNo ratings yet
- Understanding Smallpox: Causes, Symptoms and HistoryDocument24 pagesUnderstanding Smallpox: Causes, Symptoms and HistoryFahad HassanNo ratings yet
- Fluid and Elctrolyte Balance.... Power PointDocument40 pagesFluid and Elctrolyte Balance.... Power PointMarwan M.100% (1)
- Chapter 13 Diagnosing Infectious DiseasesDocument47 pagesChapter 13 Diagnosing Infectious DiseasesSherinne Jane CariazoNo ratings yet
- General Information About ScabiesDocument16 pagesGeneral Information About ScabiesPramesti DarojahNo ratings yet
- Idiopathic Thrombocytopenic Purpura (ITP)Document7 pagesIdiopathic Thrombocytopenic Purpura (ITP)Rizqka PertiwiNo ratings yet
- Sexually Transmitted InfectionsDocument34 pagesSexually Transmitted InfectionsMariana Creciun100% (1)
- Presented By: Gayramara Arben John ZDocument36 pagesPresented By: Gayramara Arben John ZgoykicoshenNo ratings yet
- Parasitology PartialDocument8 pagesParasitology Partialcayla mae carlosNo ratings yet
- Host Microbe Interactions: Understanding Virulence FactorsDocument37 pagesHost Microbe Interactions: Understanding Virulence FactorsSrijan BhattaraiNo ratings yet
- Abnormal Midwifery: by Gladys M. BSN, KRCHNDocument352 pagesAbnormal Midwifery: by Gladys M. BSN, KRCHNMercy KeruboNo ratings yet
- Sample QuestionnaireDocument10 pagesSample QuestionnaireJess Fernandez BorgaNo ratings yet
- Measles: PGI Nicole Jenne C. TanDocument40 pagesMeasles: PGI Nicole Jenne C. TanNicole Jenne TanNo ratings yet
- In The Name of Allah, The Most Beneficent and MercifulDocument35 pagesIn The Name of Allah, The Most Beneficent and MercifulAhmedMenshawyNo ratings yet
- HEPA B and PIDDocument40 pagesHEPA B and PIDNica PinedaNo ratings yet
- Pyogenic MeningitisDocument46 pagesPyogenic MeningitisShahnaaz ShahNo ratings yet
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Clinic-Pharmacologic Approaches To Antimicrobial Therapy in Surgical InfectionsDocument27 pagesClinic-Pharmacologic Approaches To Antimicrobial Therapy in Surgical InfectionsMuhammad NaveedNo ratings yet
- Maternal Sepsis and Sepsis ShockDocument17 pagesMaternal Sepsis and Sepsis ShockAlvaro Andres Flores JimenezNo ratings yet
- Vaccination or ImmunizationDocument4 pagesVaccination or ImmunizationPrincessNo ratings yet
- NCM 112: Care of Clients With Inflammatory and Immunologic Response Maricris B. Florendo/Constantino Y. Mendoza/Sandra Layne G. Luczon/Rhizza AbinsayDocument23 pagesNCM 112: Care of Clients With Inflammatory and Immunologic Response Maricris B. Florendo/Constantino Y. Mendoza/Sandra Layne G. Luczon/Rhizza AbinsayRyrey Abraham PacamanaNo ratings yet
- Surgery Papillary Thyroid CADocument15 pagesSurgery Papillary Thyroid CAMelissa LabadorNo ratings yet
- Introduction in Medical Microbiology June 2020 Online ClassDocument9 pagesIntroduction in Medical Microbiology June 2020 Online Classjames rukenyaNo ratings yet
- Vulvovaginal Candidiasis and Bacterial VaginosisDocument16 pagesVulvovaginal Candidiasis and Bacterial VaginosisAdnanda Maulan100% (1)
- Sputum CultureDocument6 pagesSputum CulturePranav Kumar PrabhakarNo ratings yet
- Linear Arrangements of DR InstrumentsDocument42 pagesLinear Arrangements of DR Instrumentsxxegyzz100% (1)
- PID: Understanding Pelvic Inflammatory DiseaseDocument34 pagesPID: Understanding Pelvic Inflammatory Diseaseraed faisalNo ratings yet
- Guidelines For Rational Use of AntibioticsDocument11 pagesGuidelines For Rational Use of AntibioticsPavitra MaheshNo ratings yet
- AppendicitiesDocument58 pagesAppendicitiesGAURAV50% (2)
- Hookworm Disease: Ancylostoma Duodenale-Are Anthropophilic Human Hookworms Transmitted From Infected SoilDocument5 pagesHookworm Disease: Ancylostoma Duodenale-Are Anthropophilic Human Hookworms Transmitted From Infected SoilBrix Valdriz100% (1)
- Communicable DiseaseDocument22 pagesCommunicable DiseaseheheeheheNo ratings yet
- CholelitiasisDocument42 pagesCholelitiasisEdwin YosuaNo ratings yet
- Filariasis in NepalDocument41 pagesFilariasis in NepalBinaya100% (1)
- Operating Room Roles and ProceduresDocument15 pagesOperating Room Roles and ProceduresRackz Glova AmaroNo ratings yet
- Amoebiasis: An Overview of Its Causes, Symptoms, Diagnosis and TreatmentDocument8 pagesAmoebiasis: An Overview of Its Causes, Symptoms, Diagnosis and TreatmentCheska ت HortelanoNo ratings yet
- Check List Suturing Aseptik - Revisi 19-01-10Document4 pagesCheck List Suturing Aseptik - Revisi 19-01-10Arief Yunan PriyoutomoNo ratings yet
- Management of Patients With Gastric and Duodenal DisordersDocument7 pagesManagement of Patients With Gastric and Duodenal DisordersintotheunknownNo ratings yet
- Roseola PDFDocument1 pageRoseola PDFLili PredescuNo ratings yet
- EINC ReviewDocument14 pagesEINC ReviewRifa'atul MahmudahNo ratings yet
- Managing Nause and Vomiting-Crit-Care-Nurse-2003-Garrett-31-50 PDFDocument22 pagesManaging Nause and Vomiting-Crit-Care-Nurse-2003-Garrett-31-50 PDFpmuftiaNo ratings yet
- Fair Use Notice and Disclaimer: OLY AME NiversityDocument12 pagesFair Use Notice and Disclaimer: OLY AME NiversityShiney Rhet DACULANo ratings yet
- Reproductive Tract InfectionDocument48 pagesReproductive Tract InfectionSampriti Roy100% (1)
- Live Preterm Baby Delivered NSDDocument13 pagesLive Preterm Baby Delivered NSDKristine Anne SorianoNo ratings yet
- Syndromic Management of Sexually Transmitted InfectionsDocument76 pagesSyndromic Management of Sexually Transmitted Infectionsnamita100% (2)
- Advancement in Partograph WHO's Labor Care GuideDocument7 pagesAdvancement in Partograph WHO's Labor Care GuideSujan ThapaNo ratings yet
- Pertussis Case Definition and Investigation PresentationDocument62 pagesPertussis Case Definition and Investigation PresentationMuhammad Jahari Supianto100% (1)
- EpisiotomyDocument16 pagesEpisiotomyRosu GeorgeNo ratings yet
- VaccinationDocument39 pagesVaccinationhaddi awanNo ratings yet
- Acute TonsillitisDocument54 pagesAcute TonsillitissuciNo ratings yet
- EBBP CompetenciesDocument11 pagesEBBP Competenciesdinger11No ratings yet
- Nursing Care of Male and Female Clients With General and Specific Problems in SexualityDocument22 pagesNursing Care of Male and Female Clients With General and Specific Problems in SexualityDecere PascualNo ratings yet
- Workplace Safety and Health Management IssuesDocument2 pagesWorkplace Safety and Health Management IssuesIsusiubestemoldovaNo ratings yet
- Certificat de Vaccinare Vaccination CertificateDocument1 pageCertificat de Vaccinare Vaccination CertificateOlga StratanNo ratings yet
- Ioesolutions Esign Com NP Contents Sanitary Engineering Ce 656Document5 pagesIoesolutions Esign Com NP Contents Sanitary Engineering Ce 656Ranjit MahatoNo ratings yet
- PB7 - Doha Declaration On TRIPS and Health - ENDocument12 pagesPB7 - Doha Declaration On TRIPS and Health - ENIshtiaque Rahman KhanNo ratings yet
- Vaccination in Special Situations SeminarDocument21 pagesVaccination in Special Situations SeminarDeep ShahNo ratings yet
- Health Pacing GuideDocument3 pagesHealth Pacing Guideapi-335323849No ratings yet
- Risk Management Case Study SelectionDocument2 pagesRisk Management Case Study SelectionPaola Quintos100% (1)
- Soc 01 Project 2 NutritionDocument13 pagesSoc 01 Project 2 Nutritionapi-354675795No ratings yet
- HCM 2337 Vector, Vermin and Rodent ControlDocument13 pagesHCM 2337 Vector, Vermin and Rodent ControlMokua FedinardNo ratings yet
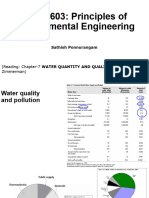
- ENEN-603 Week-7 WaterQuanQualDocument58 pagesENEN-603 Week-7 WaterQuanQualchintankp230199No ratings yet
- Instruments & IndicationsDocument11 pagesInstruments & IndicationsZiyad100% (2)
- Marabello, S., and Parisi, M. L. (2020) - I Told You The Invinsible Can Kill YouDocument10 pagesMarabello, S., and Parisi, M. L. (2020) - I Told You The Invinsible Can Kill YouMuhammad Rahul AnantaNo ratings yet
- Drawing Sanitary, PlumbingDocument1 pageDrawing Sanitary, Plumbingkhairil mohdNo ratings yet
- Registered Plumbing ContractorsDocument9 pagesRegistered Plumbing ContractorsviveknayeeNo ratings yet
- Paediatric tuberculosis assessment scoresDocument1 pagePaediatric tuberculosis assessment scoresGalaleldin AliNo ratings yet
- Evaluasi Efektivitas Terapi Pada Pasien Asma Di Rumah Sakit Khusus Paru Respira Yogyakarta Kalasan Periode November 2014 - Januari 2015Document7 pagesEvaluasi Efektivitas Terapi Pada Pasien Asma Di Rumah Sakit Khusus Paru Respira Yogyakarta Kalasan Periode November 2014 - Januari 2015Hanna PurwaningsihNo ratings yet
- COVID19 Vaccine Safety Surveillance Manual-Final EngDocument232 pagesCOVID19 Vaccine Safety Surveillance Manual-Final Engkaynabil100% (1)
- NURSING CARE PLAN FOR ACUTE GASTROENTERITISDocument6 pagesNURSING CARE PLAN FOR ACUTE GASTROENTERITISKyle VargasNo ratings yet
- Certificate for COVID-19 Vaccination in IndiaDocument1 pageCertificate for COVID-19 Vaccination in IndiaTausif KhanNo ratings yet
- Antimicrobial Dressings Made Easy PDFDocument6 pagesAntimicrobial Dressings Made Easy PDFNinaNo ratings yet
- AsepsisDocument50 pagesAsepsisVictor Juncu100% (2)
- Laboratory Safety PrecautionsDocument12 pagesLaboratory Safety PrecautionsBianca GeagoniaNo ratings yet
- SPH 596 Lecture 1 September 7 2018Document28 pagesSPH 596 Lecture 1 September 7 2018Kevin Rosen CNo ratings yet
- Student Nurses' Community: NURSING CARE PLAN Neonatal SepsisDocument2 pagesStudent Nurses' Community: NURSING CARE PLAN Neonatal SepsisChristian Remetio100% (1)
- Indiviual Rack: ProvidedDocument4 pagesIndiviual Rack: Providedkevin tomNo ratings yet
- PH Dept GosDocument160 pagesPH Dept Gosvenkatasubramaniyan100% (11)
- OMNIBUS HEALTH GUIDELINES FOR MANAGERSDocument29 pagesOMNIBUS HEALTH GUIDELINES FOR MANAGERSRaymunda Rauto-avilaNo ratings yet
- Sanitation - Wikipedia, The Free EncyclopediaDocument7 pagesSanitation - Wikipedia, The Free EncyclopediaguptaeleNo ratings yet