You might also like
- Acute Lymphoblastic LeukemiaDocument22 pagesAcute Lymphoblastic Leukemiaحسن محمدNo ratings yet
- Acute Lymphoblastic Leukemia: Maggie Davis Hovda 5/26/2009Document22 pagesAcute Lymphoblastic Leukemia: Maggie Davis Hovda 5/26/2009yuliarosiNo ratings yet
- Leukemia in ChildrenDocument44 pagesLeukemia in ChildrenSami ShouraNo ratings yet
- Acute Lymphoblastic Leukemia: Muhammad Fadhel 1410311044Document21 pagesAcute Lymphoblastic Leukemia: Muhammad Fadhel 1410311044Alvin ArifNo ratings yet
- Acute Lymphoblastic LeukemiaDocument34 pagesAcute Lymphoblastic LeukemiamtyboyNo ratings yet
- HaematologyDocument25 pagesHaematologyMenziPhiwokuhleSukatiNo ratings yet
- Acute Lymphoblastic LeukemiaDocument9 pagesAcute Lymphoblastic LeukemiaAdamant Al Johani Gangis100% (1)
- Acute Lymphoblastic Leukemia Incidence, Epidemiology, Etiology and ClassificationDocument19 pagesAcute Lymphoblastic Leukemia Incidence, Epidemiology, Etiology and ClassificationNeng AyuRati50% (2)
- Acute Myelogenous Leukemia-Aml Acute Lymphoblastic Leukemia - AllDocument64 pagesAcute Myelogenous Leukemia-Aml Acute Lymphoblastic Leukemia - AllSiraj ShiferawNo ratings yet
- Acute Lymphoblastic Leukemia - LecturioDocument17 pagesAcute Lymphoblastic Leukemia - LecturioCornel PopaNo ratings yet
- Teruko Sakurai Japanese Color Harmony DictionaryDocument22 pagesTeruko Sakurai Japanese Color Harmony DictionaryLily AddamsNo ratings yet
- Acute Leukaemia-Update: DR Niranjan N. RathodDocument89 pagesAcute Leukaemia-Update: DR Niranjan N. RathodratanNo ratings yet
- ACUTE LYMPHOBLASTIC LEUKEMIA (ALLDocument12 pagesACUTE LYMPHOBLASTIC LEUKEMIA (ALLsharon victoria mendezNo ratings yet
- Acute Lymphoblastic LeukemiaDocument5 pagesAcute Lymphoblastic LeukemiavnykumalasariNo ratings yet
- Tutorial: Section A: Multiple Choice Question (Mcqs T/F)Document7 pagesTutorial: Section A: Multiple Choice Question (Mcqs T/F)Harith AsriNo ratings yet
- WBC DisordersDocument114 pagesWBC DisordersNdor BariboloNo ratings yet
- PATHO LEC WBC Lymph Nodes Spleen Thymus Part1 CompressedDocument84 pagesPATHO LEC WBC Lymph Nodes Spleen Thymus Part1 CompressedAngelo HinonNo ratings yet
- Acute Lymphoblastic Leukemia (ALL)Document14 pagesAcute Lymphoblastic Leukemia (ALL)Med PhuongNo ratings yet
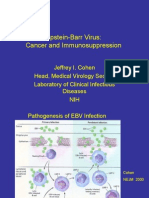
- Epstein-Barr Virus: Cancer and ImmunosuppressionDocument31 pagesEpstein-Barr Virus: Cancer and ImmunosuppressionMoisés SantosNo ratings yet
- Acute Leukemia in ChildrenDocument17 pagesAcute Leukemia in ChildrenalivanabilafarinisaNo ratings yet
- Adult Acute Lymphoblastic Leukemia: Concepts and StrategiesDocument12 pagesAdult Acute Lymphoblastic Leukemia: Concepts and StrategiesdrravesNo ratings yet
- Acute Lymphoblastic Leukemia (ALL) TreatmentDocument10 pagesAcute Lymphoblastic Leukemia (ALL) TreatmentAndreea TudurachiNo ratings yet
- Acute Leukemia HandoutDocument10 pagesAcute Leukemia Handoutnonie jacobNo ratings yet
- Acute and Chronic Leukemia FinalDocument68 pagesAcute and Chronic Leukemia FinalHannah LeiNo ratings yet
- Histiocytic Disorders Diagnosis and Treatment: Resident Education Lecture SeriesDocument41 pagesHistiocytic Disorders Diagnosis and Treatment: Resident Education Lecture SeriesChetan SekhriNo ratings yet
- Hodgkin'S Disease AND Non-Hodgkin'S LymphomaDocument42 pagesHodgkin'S Disease AND Non-Hodgkin'S LymphomaRayya TriandaNo ratings yet
- Hom 3Document7 pagesHom 3Mira SrikandiNo ratings yet
- AML, CML, ALL, CLL, HemophiliaDocument7 pagesAML, CML, ALL, CLL, HemophiliaJamara Kyla Dela CruzNo ratings yet
- Acute Lymphoblastic Leukemia: Differential DiagnosisDocument6 pagesAcute Lymphoblastic Leukemia: Differential DiagnosisIma OhwNo ratings yet
- Lymphoma: 2011-2012 Prof - Dr.Rejin Kebudi, M.DDocument57 pagesLymphoma: 2011-2012 Prof - Dr.Rejin Kebudi, M.Dmia rachmiNo ratings yet
- Acute LeukemiasDocument48 pagesAcute LeukemiaslaibaNo ratings yet
- ALL (2)Document18 pagesALL (2)pritidinda3070No ratings yet
- Case StudyDocument10 pagesCase Studysabrown109No ratings yet
- 2021 How I Treat Adult T-Cell Leukemia-LymphomaDocument12 pages2021 How I Treat Adult T-Cell Leukemia-Lymphomamateusmalacarne96No ratings yet
- Disorders of The Wihte CellsDocument22 pagesDisorders of The Wihte CellsdoniNo ratings yet
- All Aml NCCN 2023 HamidahDocument45 pagesAll Aml NCCN 2023 HamidahPPDS IPD ULMNo ratings yet
- Pa Tho Physiology of LymphomasDocument17 pagesPa Tho Physiology of LymphomasKent MasadoNo ratings yet
- Acute Lymphocytic Leukemia Treatment OverviewDocument11 pagesAcute Lymphocytic Leukemia Treatment OverviewkualamonkeyNo ratings yet
- How I Treat Essential ThrombocythemiaDocument12 pagesHow I Treat Essential ThrombocythemiaJicko Street HooligansNo ratings yet
- MCD 2015 and 2016Document6 pagesMCD 2015 and 2016Jenny LowsleyNo ratings yet
- Hodgkin's DiseaseDocument58 pagesHodgkin's Diseasealibayaty1No ratings yet
- Childhood Burkitt Lymphoma: Sabbas MDDocument35 pagesChildhood Burkitt Lymphoma: Sabbas MDLegend OMSUNo ratings yet
- Leukemia Pada AnakDocument33 pagesLeukemia Pada AnakandrianNo ratings yet
- LYMPH NODE CANCERDocument190 pagesLYMPH NODE CANCERNinna Isabel VictorioNo ratings yet
- SleDocument33 pagesSleZaira HussainNo ratings yet
- Haematopathology 3:: Leucocytosis/LeucopeniaDocument113 pagesHaematopathology 3:: Leucocytosis/LeucopeniaarwaNo ratings yet
- Myeloproliferative Disorders: Classification CML AMM PV ETDocument58 pagesMyeloproliferative Disorders: Classification CML AMM PV ETashuNo ratings yet
- Diferenciacion de Hematogonias y LinfoblastosDocument6 pagesDiferenciacion de Hematogonias y LinfoblastosSusan RamosNo ratings yet
- The LeukemiasDocument52 pagesThe Leukemiasمصطفي خندقاوي100% (1)
- Diagnostic Workup and Pathophysiology of Pre-B-Cell Acute Lymphoblastic LeukemiaDocument3 pagesDiagnostic Workup and Pathophysiology of Pre-B-Cell Acute Lymphoblastic LeukemiaNitin KumarNo ratings yet
- Acute Leukemia Types and TreatmentDocument22 pagesAcute Leukemia Types and TreatmentFelix Allen100% (1)
- Chronic Lymphocytic LeukemiaFrom EverandChronic Lymphocytic LeukemiaMichael HallekNo ratings yet
- Hemophagocytic Lymphohistiocytosis: Ranya H Albar PGY3Document38 pagesHemophagocytic Lymphohistiocytosis: Ranya H Albar PGY3Rabia AhmadNo ratings yet
- Acute Leukemia: Understanding the Pathogenesis, Diagnosis and ManagementDocument52 pagesAcute Leukemia: Understanding the Pathogenesis, Diagnosis and ManagementJamilNo ratings yet
- Acute Leukemia: Dimas Bayu Tutik Harjianti A. FachruddinDocument41 pagesAcute Leukemia: Dimas Bayu Tutik Harjianti A. FachruddinFI 034 Mega Rahmawati MaulanaNo ratings yet
- Ratheesh R.LDocument42 pagesRatheesh R.LY. Beatrice AbigailNo ratings yet
- Idiopathic Thrombocytopenic Purpura (ITP) : Feature Disease FactsDocument3 pagesIdiopathic Thrombocytopenic Purpura (ITP) : Feature Disease Factsnisa_neyshaaljufriNo ratings yet
- Acute Leukemia - Knowledge at AMBOSSDocument1 pageAcute Leukemia - Knowledge at AMBOSSRenad AlharbiNo ratings yet
- Acute Lymphoblastic Leukemia: John Han-Chih Chang Matthew M. Poppe Chia-Ho Hua Karen J. Marcus Natia EsiashviliDocument7 pagesAcute Lymphoblastic Leukemia: John Han-Chih Chang Matthew M. Poppe Chia-Ho Hua Karen J. Marcus Natia EsiashviliErvanda ZilmiNo ratings yet
- Become A Good PresenterDocument4 pagesBecome A Good PresenternoviNo ratings yet
- WHO HRH HPN 10.3 EngDocument64 pagesWHO HRH HPN 10.3 EngArif Eko YuniawanNo ratings yet
- MilkDocument104 pagesMilknoviNo ratings yet
- Repertoire of Presentation PhrasesDocument4 pagesRepertoire of Presentation Phrasesnovi100% (1)
- Essay - Should Parents Send Their Children To Preschool EducationDocument2 pagesEssay - Should Parents Send Their Children To Preschool EducationnoviNo ratings yet
- SPEAKING Book PreviewDocument70 pagesSPEAKING Book PreviewSauleSaparbekNo ratings yet
- GuidelineDocument1 pageGuidelinenoviNo ratings yet
- Case ManagementDocument9 pagesCase ManagementnoviNo ratings yet
- Handbook of Disaster Emergency Policies Institutions PDFDocument206 pagesHandbook of Disaster Emergency Policies Institutions PDFLiezty VioLen'sNo ratings yet
- Bahan 1Document19 pagesBahan 1HeidiDewiMutiaNo ratings yet
- Pengaruh Latihan Naik Turun Tangga Dan Latihan: JurnalDocument16 pagesPengaruh Latihan Naik Turun Tangga Dan Latihan: JurnalAprilian SandiNo ratings yet
- Respiratory Tract DisorderDocument30 pagesRespiratory Tract DisordernoviNo ratings yet
- ProQuestDocuments 2017-04-26Document13 pagesProQuestDocuments 2017-04-26noviNo ratings yet
- Acute Lymphoblastic Leukemia Treatment OverviewDocument22 pagesAcute Lymphoblastic Leukemia Treatment OverviewnoviNo ratings yet
- Bahan 1Document19 pagesBahan 1HeidiDewiMutiaNo ratings yet
- Annsurg00088 0120Document10 pagesAnnsurg00088 0120noviNo ratings yet
- Aphn Roleofphnindisasterprr Finaljan14 QBD 5Document19 pagesAphn Roleofphnindisasterprr Finaljan14 QBD 5noviNo ratings yet
- Correlation of Breast Cancer Incidence With Motor Vehicles and Consumption of Gasoline in KoreaDocument6 pagesCorrelation of Breast Cancer Incidence With Motor Vehicles and Consumption of Gasoline in KoreanoviNo ratings yet
- OD-PRO-HSE-032 Safety To Work at Height - Rev.01Document31 pagesOD-PRO-HSE-032 Safety To Work at Height - Rev.01aymenmoataz100% (1)
- Social Relationships in Middle and Late AdolescentDocument9 pagesSocial Relationships in Middle and Late AdolescentNesta Norhyl BayonaNo ratings yet
- Quality Assurance in Medical LaboratoriesDocument69 pagesQuality Assurance in Medical Laboratories"DocAxi" Maximo B Axibal Jr MD FPSP100% (1)
- Summary Water Treatment PlantDocument4 pagesSummary Water Treatment PlantDalil Nur FarahaniNo ratings yet
- Patella FractureDocument52 pagesPatella FractureM Jalil khanNo ratings yet
- MSDS - CRC Seal Coat ® Urethane Coating - ClearDocument3 pagesMSDS - CRC Seal Coat ® Urethane Coating - ClearLailal HaqimNo ratings yet
- READING ON Tick-Borne DiseasesDocument3 pagesREADING ON Tick-Borne DiseasesMonique LeonardoNo ratings yet
- The Star News November 20, 2014Document37 pagesThe Star News November 20, 2014The Star NewsNo ratings yet
- Fibre Cement Slates Fixing GuideDocument26 pagesFibre Cement Slates Fixing GuideMuhammad HafizuddinNo ratings yet
- Interim Public Health Operational Guidelines For Amoebiasis: (Entamoeba Histolytica)Document34 pagesInterim Public Health Operational Guidelines For Amoebiasis: (Entamoeba Histolytica)QworldNo ratings yet
- Learning Kit - Q3W3 CeslDocument10 pagesLearning Kit - Q3W3 CeslJoselle Batas MagbanuaNo ratings yet
- MRNA Vaccines - Day - 04.14.20 PDFDocument259 pagesMRNA Vaccines - Day - 04.14.20 PDFTammy G100% (1)
- Admin of Meds Prof GuidanceDocument8 pagesAdmin of Meds Prof GuidanceStacyNo ratings yet
- ACTION PLAN FOR JUVENILE PRISONERS IN ILOILO CITYDocument22 pagesACTION PLAN FOR JUVENILE PRISONERS IN ILOILO CITYJohn Christian LopezNo ratings yet
- Argumentative Essay (Yasmin Claire T. Navarro)Document2 pagesArgumentative Essay (Yasmin Claire T. Navarro)Yasmin Claire NavarroNo ratings yet
- Fire Safety Fundamentals and Fire Extinguisher ClassificationsDocument3 pagesFire Safety Fundamentals and Fire Extinguisher ClassificationsGangapuram SrikanthNo ratings yet
- Reflective Essay: Writing in The Genetics DiscourseDocument5 pagesReflective Essay: Writing in The Genetics DiscourseAnonymous AY6XDZHBxPNo ratings yet
- Acd Iam 05 ImatDocument2 pagesAcd Iam 05 Imatnjk realty100% (1)
- Paragraph TypesDocument4 pagesParagraph TypesZayb EhmadNo ratings yet
- Benefits of Effective Lifting ProgramDocument30 pagesBenefits of Effective Lifting ProgramMoradeke OnasanyaNo ratings yet
- Igem ListDocument9 pagesIgem ListMilad YadollahiNo ratings yet
- Douglas Crucey, A043 446 797 (BIA June 12, 2017)Document20 pagesDouglas Crucey, A043 446 797 (BIA June 12, 2017)Immigrant & Refugee Appellate Center, LLCNo ratings yet
- Coping Strategies of Athletes for Competitive AnxietyDocument13 pagesCoping Strategies of Athletes for Competitive AnxietyHONEY JEAN ESPENORIONo ratings yet
- Single/ Exam Zone Centre DetailsDocument5 pagesSingle/ Exam Zone Centre DetailsHarsh AroraNo ratings yet
- Eclampsia Nursing Care Plan - Altered Tissue PerfusionDocument2 pagesEclampsia Nursing Care Plan - Altered Tissue PerfusionCyrus De Asis84% (32)
- Remember: Blood CirculationDocument4 pagesRemember: Blood CirculationvicpardoNo ratings yet
- Managing Employee Attitudes and Well-BeingDocument2 pagesManaging Employee Attitudes and Well-BeingJayChristian QuimsonNo ratings yet
- Juvenile Rheumatoid Arthritis: Dorothy W. Wortmann, MDDocument38 pagesJuvenile Rheumatoid Arthritis: Dorothy W. Wortmann, MDLavi GoyalNo ratings yet
- Main - Factsheet Tacrolimus OintmentDocument4 pagesMain - Factsheet Tacrolimus OintmentSakuranbochanNo ratings yet
- Changes in Demand and Supply of Face Masks Under CovidDocument3 pagesChanges in Demand and Supply of Face Masks Under CovidHanh HoangNo ratings yet