You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Med Trans ReviewerDocument1 pageMed Trans ReviewerDenise CerdaNo ratings yet
- BPE109 Module 2.2 Musculoskeletal System PDFDocument7 pagesBPE109 Module 2.2 Musculoskeletal System PDFZedy GullesNo ratings yet
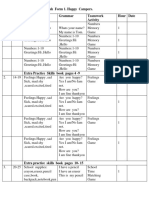
- English Form 1. Happy Campers. Unit Pages Vocabulary Grammar Teamwork Activity Hour DateDocument4 pagesEnglish Form 1. Happy Campers. Unit Pages Vocabulary Grammar Teamwork Activity Hour Dateİlkanə CabbarovaNo ratings yet
- Brain Training Dogs (Develops Your Dog's "Hidden Intelligence")Document16 pagesBrain Training Dogs (Develops Your Dog's "Hidden Intelligence")JohnNo ratings yet
- AMCAT CocubesDocument35 pagesAMCAT CocubesMuthyala Akhil100% (6)
- Arcanis Children of The Sky The Kio SourcebookDocument68 pagesArcanis Children of The Sky The Kio SourcebookMatthew AperNo ratings yet
- The Crane Frolics: The Path From Qihai To TanzhongDocument4 pagesThe Crane Frolics: The Path From Qihai To Tanzhongapi-268467409100% (1)
- Pre Columbian Art Including Selection of LempertzDocument148 pagesPre Columbian Art Including Selection of LempertzAQQUIROGA50% (2)
- Lecture 5. Gas Exchange: Cellular Respiration, Oxidative Processes Within External Respiration, Exchange of O2 and CO2Document24 pagesLecture 5. Gas Exchange: Cellular Respiration, Oxidative Processes Within External Respiration, Exchange of O2 and CO2Jay JayNo ratings yet
- Bangladesh: NiversityDocument50 pagesBangladesh: Niversitylokesh kumarNo ratings yet
- Classis Reptilia Ordo TestudinataDocument14 pagesClassis Reptilia Ordo TestudinataAnang Yanuar RamadhanNo ratings yet
- Keep Up With Feeding And/or Pasture Management. You Cannot Raise Cattle If You Have Nothing To Feed Them orDocument8 pagesKeep Up With Feeding And/or Pasture Management. You Cannot Raise Cattle If You Have Nothing To Feed Them orMarie Lyca Dela CruzNo ratings yet
- World's Most Awesome Invertebrate: Activity Subject: Invertebrate Biodiversity Grade Level: 7 - 12 GradesDocument5 pagesWorld's Most Awesome Invertebrate: Activity Subject: Invertebrate Biodiversity Grade Level: 7 - 12 GradesVeraNo ratings yet
- Neonatal Sepsis: Ekawaty Lutfia Haksari Perinatology, Department of Child Health Gadjah Mada UniversityDocument28 pagesNeonatal Sepsis: Ekawaty Lutfia Haksari Perinatology, Department of Child Health Gadjah Mada Universityireneaurelia100% (1)
- Daily Reading Book 1 PDFDocument11 pagesDaily Reading Book 1 PDFSanjeevan SivapaleswararajahNo ratings yet
- Radiographic Positioning SummaryDocument10 pagesRadiographic Positioning SummaryCindy100% (1)
- Tajweed Course - Articulation PointsDocument30 pagesTajweed Course - Articulation PointsNasrin AktherNo ratings yet
- Chapter 18. LaryngoscopesDocument133 pagesChapter 18. Laryngoscopesadham08No ratings yet
- Bull Terrier Kills ChildDocument1 pageBull Terrier Kills ChildsallyfrankenwarteNo ratings yet
- Hematology 1 MidtermsDocument31 pagesHematology 1 Midtermsella SyNo ratings yet
- African Grey Parrot - WikipediaDocument3 pagesAfrican Grey Parrot - WikipediaWilhelm Richard WagnerNo ratings yet
- Soal SD Kelas 6 Semester 1Document13 pagesSoal SD Kelas 6 Semester 1fadli yasyaNo ratings yet
- فرهنگ شمس اللغات - نیمه دومDocument936 pagesفرهنگ شمس اللغات - نیمه دومamsj100% (2)
- Cat - Wikipedia PDFDocument6 pagesCat - Wikipedia PDFGodha KiranaNo ratings yet
- Oxford Discover 2. SB. Transcripts Listening Sect. - 2019Document6 pagesOxford Discover 2. SB. Transcripts Listening Sect. - 2019Mon Abdel SalamNo ratings yet
- Explorers 4 Unit 6 Under The Sea 2Document3 pagesExplorers 4 Unit 6 Under The Sea 2Gregorio CuadradoNo ratings yet
- Sarnat Scoring Tool: Normal/Mild Moderate HIE Severe HIEDocument1 pageSarnat Scoring Tool: Normal/Mild Moderate HIE Severe HIEBilly WijayaNo ratings yet
- Introduction To Dermatology: DR D J Barker ST Luke's Hospital, BradfordDocument47 pagesIntroduction To Dermatology: DR D J Barker ST Luke's Hospital, BradfordSilviuNo ratings yet
- Listening - Compare Animal and Human Behavior 2 - Mode - Report - Unit 6 - Lesson 3 - Vantage B2 - MyEnglishLabDocument1 pageListening - Compare Animal and Human Behavior 2 - Mode - Report - Unit 6 - Lesson 3 - Vantage B2 - MyEnglishLabAnnuar Florez100% (1)
- Sinelnikov Vol IIDocument436 pagesSinelnikov Vol IIOana Musteaţǎ95% (59)