You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Local Anaesthetic Doses Guidance - NCH OnlyDocument2 pagesLocal Anaesthetic Doses Guidance - NCH OnlyakshayNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Peran Perawat Dalam Penangan Kegawatn Jantung - ERWIN (Autosaved)Document64 pagesPeran Perawat Dalam Penangan Kegawatn Jantung - ERWIN (Autosaved)Adrianus AdrianusNo ratings yet
- IJGM 310577 Modified Chest X Ray Scoring System in Evaluating Severity oDocument6 pagesIJGM 310577 Modified Chest X Ray Scoring System in Evaluating Severity oApriany Fitri SangajiNo ratings yet
- 0812 Gelofusine PDFDocument2 pages0812 Gelofusine PDFMsglow WulanNo ratings yet
- UnderstandingAnesthesia1 1 2Document144 pagesUnderstandingAnesthesia1 1 2marina_shawkyNo ratings yet
- TIVA Technique For Ambulatory AnesthesiaDocument5 pagesTIVA Technique For Ambulatory AnesthesiaApriany Fitri SangajiNo ratings yet
- FemoralvesselspaperDocument6 pagesFemoralvesselspaperApriany Fitri SangajiNo ratings yet
- Ventricular ExtrasystolesDocument3 pagesVentricular ExtrasystolesApriany Fitri SangajiNo ratings yet
- 2015 ESC-ERS Gles PH-Web Addenda-Ehv317Document13 pages2015 ESC-ERS Gles PH-Web Addenda-Ehv317WennyNo ratings yet
- Hopkins 2009Document6 pagesHopkins 2009Muhammad Irvan AvandiNo ratings yet
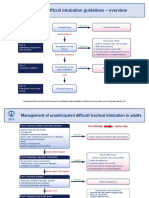
- Difficult Intubation Guidelines OverviewDocument3 pagesDifficult Intubation Guidelines OverviewMaufer AlNo ratings yet
- Epidural Analgesia in Critically Ill Patients With Acute Pancreatitis: The Multicentre Randomised Controlled EPIPAN Study ProtocolDocument10 pagesEpidural Analgesia in Critically Ill Patients With Acute Pancreatitis: The Multicentre Randomised Controlled EPIPAN Study ProtocolApriany Fitri SangajiNo ratings yet
- PERIOPERATIVE CARE ISSUES AND PHILOSOPHYDocument17 pagesPERIOPERATIVE CARE ISSUES AND PHILOSOPHYApriany Fitri SangajiNo ratings yet
- Managing Allergic Rhinitis in ChildrenDocument23 pagesManaging Allergic Rhinitis in ChildrenApriany Fitri SangajiNo ratings yet
- PERIOPERATIVE CARE ISSUES AND PHILOSOPHYDocument17 pagesPERIOPERATIVE CARE ISSUES AND PHILOSOPHYApriany Fitri SangajiNo ratings yet
- Antibiotics in Critically Ill E4ED FinalDocument46 pagesAntibiotics in Critically Ill E4ED FinalApriany Fitri SangajiNo ratings yet
- Isicm - Fccs .Brochure - OptDocument2 pagesIsicm - Fccs .Brochure - OptSofinaKusnadiNo ratings yet
- DR Badriul HegarDocument14 pagesDR Badriul HegarApriany Fitri SangajiNo ratings yet
- Diagnosis Pneumonia: M Sidhartani ZainDocument28 pagesDiagnosis Pneumonia: M Sidhartani ZainApriany Fitri SangajiNo ratings yet
- Pain Management in EDDocument40 pagesPain Management in EDscribdmihNo ratings yet
- SSC Statements Sepsis Definitions 3 2016Document2 pagesSSC Statements Sepsis Definitions 3 2016Satbir SinghNo ratings yet
- DepEd Medical CertificateDocument1 pageDepEd Medical CertificateMaria Eleonor C. BañaresNo ratings yet
- Comparison of UMN & LMN SyndromesDocument2 pagesComparison of UMN & LMN SyndromesPJHGNo ratings yet
- Diseases of The Immune System: OBC 231 General PathologyDocument91 pagesDiseases of The Immune System: OBC 231 General PathologyRana MohammadNo ratings yet
- G 098 DatasetforthyroidcancerhistopathologyreportsfinalDocument21 pagesG 098 DatasetforthyroidcancerhistopathologyreportsfinalCarloscharlieranaNo ratings yet
- Chestionar Perfectionism in The Self and Social ContextsDocument15 pagesChestionar Perfectionism in The Self and Social Contexts119568No ratings yet
- Yemisi Chapter ThreeDocument10 pagesYemisi Chapter ThreeAbimbola OyarinuNo ratings yet
- Ante Saccharomyces CerevisiaeDocument29 pagesAnte Saccharomyces CerevisiaeMichelle Efren-LabantaNo ratings yet
- Standard Precautions Hand Hygiene Gloves GownsDocument4 pagesStandard Precautions Hand Hygiene Gloves GownsAjeesh GopidasanNo ratings yet
- Pressure Ulcer PreventionDocument4 pagesPressure Ulcer PreventionJoão SantosNo ratings yet
- Ana Liezl Mendoza Illescas1 1 1 1Document3 pagesAna Liezl Mendoza Illescas1 1 1 1Prinze SereguineNo ratings yet
- Aplastic AnemiaDocument7 pagesAplastic Anemianeil052288% (8)
- Satelec Tip Book 2011Document9 pagesSatelec Tip Book 2011akash_81087No ratings yet
- ZANARINI RATING SCALE FOR BORDERLINE Zanarini2003 PDFDocument10 pagesZANARINI RATING SCALE FOR BORDERLINE Zanarini2003 PDFCesar CantaruttiNo ratings yet
- RBCDH: Methods For Estimating Body Weight and Height in Hospitalized Adults: A Comparative AnalysisDocument10 pagesRBCDH: Methods For Estimating Body Weight and Height in Hospitalized Adults: A Comparative AnalysisBoh Cucu KaraengNo ratings yet
- Snapshot NCP Step 3 Nutrition Intervention-1Document1 pageSnapshot NCP Step 3 Nutrition Intervention-1api-250924915No ratings yet
- Time To Learn. Understanding Patient Centered CareDocument7 pagesTime To Learn. Understanding Patient Centered CareAden DhenNo ratings yet
- GHJKKDocument759 pagesGHJKKVu HauNo ratings yet
- DreamsDocument52 pagesDreamsNill SalunkeNo ratings yet
- Brenda MilnerDocument8 pagesBrenda Milneryuritrujillo33No ratings yet
- Defining Traction and Fixation TermsDocument25 pagesDefining Traction and Fixation Termsmftaganas100% (1)
- Kaiser Permanente California Plans and Benefits Brochure KPIF 2011Document6 pagesKaiser Permanente California Plans and Benefits Brochure KPIF 2011DennisNo ratings yet
- ShockDocument33 pagesShockVijith.V.kumarNo ratings yet
- Breast Mass GuideDocument20 pagesBreast Mass GuideFabian Ramirez HincapiéNo ratings yet
- Staff Nurse Evaluation FormDocument1 pageStaff Nurse Evaluation FormCandy QuijanoNo ratings yet
- Csi - Glenda LongoriaDocument11 pagesCsi - Glenda Longoriaapi-302707617No ratings yet
- NTSB LIRR ReportDocument26 pagesNTSB LIRR ReportNewsdayNo ratings yet
- Vital Sign IpgDocument2 pagesVital Sign Ipgapi-351581044No ratings yet
- Transitional Care: DR - Vinoli.S.G Professor HOD Medical Surgical Nursing Dept Universal College of Nursing BangaloreDocument15 pagesTransitional Care: DR - Vinoli.S.G Professor HOD Medical Surgical Nursing Dept Universal College of Nursing BangalorevinoliNo ratings yet
- Traditional Filipino healing practices and beliefsDocument70 pagesTraditional Filipino healing practices and beliefsJennifer BolongNo ratings yet