You might also like
- Health Information System Developmen T (Medical Records)Document21 pagesHealth Information System Developmen T (Medical Records)skidz137217100% (10)
- Quality CircleDocument33 pagesQuality CircleSudeesh SudevanNo ratings yet
- English Skills BookDocument49 pagesEnglish Skills BookAngela SpadeNo ratings yet
- LLoyd's Register Marine - Global Marine Safety TrendsDocument23 pagesLLoyd's Register Marine - Global Marine Safety Trendssuvabrata_das01100% (1)
- Explaining GenogramsDocument4 pagesExplaining GenogramsNadira Farah Prayogo100% (5)
- 4.krisis Hipertensi IMELS 15Document41 pages4.krisis Hipertensi IMELS 15putusanggraNo ratings yet
- Penyakit Ginjal Kronik Dan Indikasi Dialisis DR Ratih Tri KD MAJUDocument56 pagesPenyakit Ginjal Kronik Dan Indikasi Dialisis DR Ratih Tri KD MAJUFitriana WijayatiNo ratings yet
- Komplikasi Akut DM - Dr. RensaDocument42 pagesKomplikasi Akut DM - Dr. RensaLeonardus William KuswaraNo ratings yet
- Surviving Sepsis CampaignDocument16 pagesSurviving Sepsis CampaignKHAIRUL REDZUANNo ratings yet
- Interpretasi Urine RutinDocument118 pagesInterpretasi Urine Rutinboy jendri huluNo ratings yet
- TiroidDocument26 pagesTiroidJoni Riana MustaqimNo ratings yet
- Acut Coronary Syndrome: Joko Sutrisno, S.Kep, NsDocument54 pagesAcut Coronary Syndrome: Joko Sutrisno, S.Kep, NsJokoSutrisnoNo ratings yet
- Hypertension Urgency and EmergencyDocument8 pagesHypertension Urgency and EmergencySanditia GumilangNo ratings yet
- Perioperative Management in Diabetes MellitusDocument20 pagesPerioperative Management in Diabetes MellitusChristopher RyalinoNo ratings yet
- Hipertensi-Krisis Dr. HendroDocument35 pagesHipertensi-Krisis Dr. Hendroyudhagp100% (1)
- Management of Diabetes Mellitus in Surgical PatientsDocument12 pagesManagement of Diabetes Mellitus in Surgical PatientsAnggoro Bayu Agung DjangkaruNo ratings yet
- Nutritional Management for Patients with Chronic Kidney DiseaseDocument41 pagesNutritional Management for Patients with Chronic Kidney DiseaseZaza ZunitaNo ratings yet
- Hyperosmolar Hyperglycemic StateDocument13 pagesHyperosmolar Hyperglycemic Stateanon_903760906No ratings yet
- The Rich Hues of Purple Murex DyeDocument44 pagesThe Rich Hues of Purple Murex DyeYiğit KılıçNo ratings yet
- Diagnosa & Tatalaksana DiabetesDocument46 pagesDiagnosa & Tatalaksana DiabetesAdhelia Kusuma WardhaniNo ratings yet
- Chronic Liver DiseaseDocument3 pagesChronic Liver DiseaseMohammad AbbasNo ratings yet
- WS 5 - DR DR C Heriawan Soejono, SPPD, KGer, M.Epid, MPH - TATALAKSANA PASIEN GERIATRI PDFDocument34 pagesWS 5 - DR DR C Heriawan Soejono, SPPD, KGer, M.Epid, MPH - TATALAKSANA PASIEN GERIATRI PDFApres SyahwaNo ratings yet
- Gasem MH HANTA Salatiga 2019Document43 pagesGasem MH HANTA Salatiga 2019ChristianNo ratings yet
- Revisi CKD On HDDocument43 pagesRevisi CKD On HDMaladewi RofyNo ratings yet
- COPD and Pneumonia Case ReportDocument23 pagesCOPD and Pneumonia Case ReportbahrinaNo ratings yet
- Kul Sem 4 Heat Stroke N Fever UHT 2016Document63 pagesKul Sem 4 Heat Stroke N Fever UHT 2016NandaSuryaWijayaNo ratings yet
- S1.1 Ria Bandiara - Role Managemen Hypertension PKB 2019Document29 pagesS1.1 Ria Bandiara - Role Managemen Hypertension PKB 2019siputleletNo ratings yet
- REFERAT DMARDsDocument42 pagesREFERAT DMARDsBhayu Dharma SuryanaNo ratings yet
- Managing Acute Metabolic Complications of Diabetes: HHS TreatmentDocument24 pagesManaging Acute Metabolic Complications of Diabetes: HHS TreatmentAnnisaNo ratings yet
- SEO-Optimized Title for PBC Case ReportDocument40 pagesSEO-Optimized Title for PBC Case Reportv_vijayakanth7656No ratings yet
- Bimbingan Dokter Hari - CKDDocument24 pagesBimbingan Dokter Hari - CKDVicky LumalessilNo ratings yet
- Algoritma HipokalsemiaDocument1 pageAlgoritma HipokalsemiaAnsilNo ratings yet
- Diabetes IdiDocument71 pagesDiabetes IdiAriyanaNo ratings yet
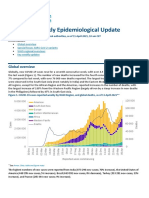
- COVID-19 Weekly Epidemiological Update: Global OverviewDocument31 pagesCOVID-19 Weekly Epidemiological Update: Global OverviewPaolaNo ratings yet
- Dr. Erlieza Roosdhania, SP - PD (CKD)Document38 pagesDr. Erlieza Roosdhania, SP - PD (CKD)Pon PondNo ratings yet
- Diabetes Mellitus: DR Hiew Fu LiongDocument30 pagesDiabetes Mellitus: DR Hiew Fu LiongamminsaffriNo ratings yet
- Chronic Heart FailureDocument25 pagesChronic Heart FailureNeilavery WindaNo ratings yet
- Manage Anemia in CKD Patients: Iron Therapy GuidelinesDocument36 pagesManage Anemia in CKD Patients: Iron Therapy GuidelinesLaurensia Erlina NataliaNo ratings yet
- Pemeriksaan Laboratorium HatiDocument67 pagesPemeriksaan Laboratorium HatiTutde SedanaNo ratings yet
- Tatalaksana Hipertensi EmergensiDocument31 pagesTatalaksana Hipertensi EmergensiSitiMaghfirahHafizNo ratings yet
- Medical Check Up: Cek KesehatanDocument20 pagesMedical Check Up: Cek KesehatanEmi PephiNo ratings yet
- Pembahasan To 1 (Patof) Batch Feb 2016Document718 pagesPembahasan To 1 (Patof) Batch Feb 2016ilmupengetahuanNo ratings yet
- Tutorial Klinik Stase Ilmu Penyakit Dalam: GastrohepatologiDocument48 pagesTutorial Klinik Stase Ilmu Penyakit Dalam: GastrohepatologiMerry MiraNo ratings yet
- SNMPTN 2015 IPB ResultsDocument2,279 pagesSNMPTN 2015 IPB Resultsingridpanbara0% (1)
- Nutrisi - Dr. Afiatin PDFDocument68 pagesNutrisi - Dr. Afiatin PDFekorahmanadiNo ratings yet
- FINAL Management Update of Hyperuricemia & GoutDocument50 pagesFINAL Management Update of Hyperuricemia & GoutNeni Septria NingsihNo ratings yet
- 1st Announcemen LIVER UPDATE 2021 - NEW12jan21Document10 pages1st Announcemen LIVER UPDATE 2021 - NEW12jan21FebrianNo ratings yet
- Modul 4 Urin Incontinence: Group 14 Problem Base Learning Medical Faculty Muslim University of IndonesiaDocument22 pagesModul 4 Urin Incontinence: Group 14 Problem Base Learning Medical Faculty Muslim University of IndonesiaYhaya 'Dzulhijjahyanti'No ratings yet
- Anemia in Chronic Kidney DiseaseDocument38 pagesAnemia in Chronic Kidney DiseaseHemodialisa LindimaraNo ratings yet
- Left Ventricular Hyperthrophy CriteriaDocument2 pagesLeft Ventricular Hyperthrophy CriteriaDya AndryanNo ratings yet
- Albumin in Liver Cirrhosis, SADocument37 pagesAlbumin in Liver Cirrhosis, SADwinita ViviantiNo ratings yet
- Anemia in CKD and DialysisDocument38 pagesAnemia in CKD and Dialysisapoorva jainNo ratings yet
- Slide Chronic Pain-Rudy Hidayat-Iai PDFDocument30 pagesSlide Chronic Pain-Rudy Hidayat-Iai PDFAsri ArrachmanNo ratings yet
- Jambore-Pkb (Lazuardi Dwipa, DR - SPPD, K-Ger)Document65 pagesJambore-Pkb (Lazuardi Dwipa, DR - SPPD, K-Ger)UPT PKM UJUNGBERUNG INDAHNo ratings yet
- INSULIN AND ORAL HYPOGLYCEMIC AGENTSDocument35 pagesINSULIN AND ORAL HYPOGLYCEMIC AGENTSSwietenia Rambu SabatiNo ratings yet
- Uremic LungDocument26 pagesUremic LungCitra Wulandari SofyanNo ratings yet
- Chronic Kidney Disease Stages, Risk Factors, and TreatmentDocument45 pagesChronic Kidney Disease Stages, Risk Factors, and Treatmentnaro ayosNo ratings yet
- Anaphylaxis GuideDocument27 pagesAnaphylaxis Guidenadya idfentiNo ratings yet
- Spektrum AIDocument55 pagesSpektrum AIOgizWaraNo ratings yet
- Sindrom KardiorenalDocument12 pagesSindrom KardiorenalAndreAHutasoitNo ratings yet
- AN AIDS PATIENT WITH CRYPTOCOCCUS NEOFORMANS PNEUMONIADocument26 pagesAN AIDS PATIENT WITH CRYPTOCOCCUS NEOFORMANS PNEUMONIABrinna Anindita SatriaNo ratings yet
- Laporan Kasus StemiDocument41 pagesLaporan Kasus StemiNur Aisyah Soedarmin IieychaNo ratings yet
- PansitopeniaDocument33 pagesPansitopeniaBrad WrightNo ratings yet
- WAFB, WAHP, WAVV Airport ChartDocument4 pagesWAFB, WAHP, WAVV Airport ChartAbang Fayyad0% (1)
- Teori Obat DispepsiaDocument13 pagesTeori Obat DispepsiaPasti SuksesNo ratings yet
- Update On BCAA PDFDocument26 pagesUpdate On BCAA PDFdr Iyan DarmawanNo ratings yet
- Septic PatientDocument12 pagesSeptic PatientDebby Christiana SNo ratings yet
- 581 PDFDocument64 pages581 PDFkookiescreamNo ratings yet
- Chapter4 Mechanism of Action of Hormones That Act On Nuclear ReceptorsDocument11 pagesChapter4 Mechanism of Action of Hormones That Act On Nuclear ReceptorsDebby Christiana SNo ratings yet
- Chapter2 Clinical EndocrinologyDocument17 pagesChapter2 Clinical EndocrinologyDebby Christiana SNo ratings yet
- 581 PDFDocument64 pages581 PDFkookiescreamNo ratings yet
- Chapter1 Principles of Endocrinology PDFDocument10 pagesChapter1 Principles of Endocrinology PDFDebby Christiana SNo ratings yet
- Septic PatientDocument12 pagesSeptic PatientDebby Christiana SNo ratings yet
- Hyperglycemia and DM in Patient With Schizophrenia or Schizoaffective DisorderDocument6 pagesHyperglycemia and DM in Patient With Schizophrenia or Schizoaffective DisorderDebby Christiana SNo ratings yet
- Chapter2 Clinical EndocrinologyDocument17 pagesChapter2 Clinical EndocrinologyDebby Christiana SNo ratings yet
- Prevalence Pituitary AdenomaDocument7 pagesPrevalence Pituitary AdenomaDebby Christiana SNo ratings yet
- Thyroid Exec SummDocument40 pagesThyroid Exec SummKelly Posadas-MesinaNo ratings yet
- Clinical Outcome After Surgery of Pituitary AdenomaDocument7 pagesClinical Outcome After Surgery of Pituitary AdenomaDebby Christiana SNo ratings yet
- Thyroid GuidelinesDocument43 pagesThyroid GuidelinesNathaly LapoNo ratings yet
- Mechanisms and Treatment of Hypercalcemia of MalignancyDocument8 pagesMechanisms and Treatment of Hypercalcemia of MalignancyDebby Christiana SNo ratings yet
- Acls DrugsDocument5 pagesAcls DrugsDebby Christiana SNo ratings yet
- PTH and Osteoporosis in MenDocument8 pagesPTH and Osteoporosis in MenDebby Christiana SNo ratings yet
- Guidelines TBC TerbaruDocument160 pagesGuidelines TBC TerbaruSutoto MoeljadiNo ratings yet
- DM Guidelines CCPDocument53 pagesDM Guidelines CCPChristian JaraNo ratings yet
- Java MCQ QuestionsDocument11 pagesJava MCQ QuestionsPineappleNo ratings yet
- The Impact of Information Technology and Innovation To Improve Business Performance Through Marketing Capabilities in Online Businesses by Young GenerationsDocument10 pagesThe Impact of Information Technology and Innovation To Improve Business Performance Through Marketing Capabilities in Online Businesses by Young GenerationsLanta KhairunisaNo ratings yet
- CH - 3Document3 pagesCH - 3Phantom GamingNo ratings yet
- Merchandise Floor Ready Standards - Supplier InformationDocument46 pagesMerchandise Floor Ready Standards - Supplier InformationGarmentLearner100% (1)
- CCEE SWD Basic Levers ToolDocument28 pagesCCEE SWD Basic Levers ToolDivina Margarita Gómez AlvarengaNo ratings yet
- Chetan Bhagat's "Half GirlfriendDocument4 pagesChetan Bhagat's "Half GirlfriendDR Sultan Ali AhmedNo ratings yet
- 3 Steel Grating Catalogue 2010 - SERIES 1 PDFDocument6 pages3 Steel Grating Catalogue 2010 - SERIES 1 PDFPablo MatrakaNo ratings yet
- RestrukturisasiDocument17 pagesRestrukturisasimuhammad hayel wallaNo ratings yet
- Prof. Michael Murray - Some Differential Geometry ExercisesDocument4 pagesProf. Michael Murray - Some Differential Geometry ExercisesAnonymous 9rJe2lOskxNo ratings yet
- Fda PDFDocument2 pagesFda PDFVictorNo ratings yet
- Principles of Cost Accounting 1Document6 pagesPrinciples of Cost Accounting 1Alimamy KamaraNo ratings yet
- E Learning: A Student Guide To MoodleDocument16 pagesE Learning: A Student Guide To MoodleHaytham Abdulla SalmanNo ratings yet
- DANZIG, Richard, A Comment On The Jurisprudence of The Uniform Commercial Code, 1975 PDFDocument17 pagesDANZIG, Richard, A Comment On The Jurisprudence of The Uniform Commercial Code, 1975 PDFandresabelrNo ratings yet
- Intec Waste PresiDocument8 pagesIntec Waste Presiapi-369931794No ratings yet
- EQ - Module - Cantilever MethodDocument17 pagesEQ - Module - Cantilever MethodAndrea MalateNo ratings yet
- Dell EMC VPLEX For All-FlashDocument4 pagesDell EMC VPLEX For All-Flashghazal AshouriNo ratings yet
- Drypro832 PreInstallGude 0921YH220B 070627 FixDocument23 pagesDrypro832 PreInstallGude 0921YH220B 070627 FixRicardoNo ratings yet
- Learning Online: Veletsianos, GeorgeDocument11 pagesLearning Online: Veletsianos, GeorgePsico XavierNo ratings yet
- Startups Helping - India Go GreenDocument13 pagesStartups Helping - India Go Greensimran kNo ratings yet
- Research Paper Theory of Mind 2Document15 pagesResearch Paper Theory of Mind 2api-529331295No ratings yet
- Maximizing modular learning opportunities through innovation and collaborationDocument2 pagesMaximizing modular learning opportunities through innovation and collaborationNIMFA SEPARANo ratings yet
- Hydrotest CalculationDocument1 pageHydrotest CalculationkiranNo ratings yet
- AP Euro Unit 2 Study GuideDocument11 pagesAP Euro Unit 2 Study GuideexmordisNo ratings yet
- Impact of Recruitment & Selection on Employee RetentionDocument39 pagesImpact of Recruitment & Selection on Employee RetentiongizawNo ratings yet
- Body Scan AnalysisDocument9 pagesBody Scan AnalysisAmaury CosmeNo ratings yet