You might also like
- ZOO 4733 - Exam 2 ReviewDocument25 pagesZOO 4733 - Exam 2 ReviewDaniel PóoNo ratings yet
- Companion Quartet Book 1 - The Secret of The SirensDocument168 pagesCompanion Quartet Book 1 - The Secret of The Sirensadelene60% (5)
- Urinary Tract InfectionDocument10 pagesUrinary Tract InfectionMira Mariana UlfahNo ratings yet
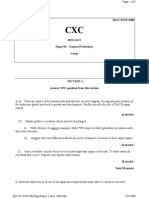
- 2000 CXC Biology Paper 3 - May-JunDocument4 pages2000 CXC Biology Paper 3 - May-JunSaintm101100% (2)
- VictoriaBoutenko 12 Steps To Raw Foods How To End Your Dependency On Cooked Food TextDocument94 pagesVictoriaBoutenko 12 Steps To Raw Foods How To End Your Dependency On Cooked Food Textmichelleyeohfan100% (2)
- Brain Boosting Activities For KidsDocument48 pagesBrain Boosting Activities For KidsMiss Kelly100% (5)
- Madcow and Mad "Human" DiseaseDocument15 pagesMadcow and Mad "Human" DiseaseMaruli PandjaitanNo ratings yet
- Urinary Tract Infection (UTI) : Omega Mellyana Sub Bag. Nefrologi Anak FK UNDIP-RSUP Dr. KariadiDocument24 pagesUrinary Tract Infection (UTI) : Omega Mellyana Sub Bag. Nefrologi Anak FK UNDIP-RSUP Dr. KariadiRastia AlimmattabrinaNo ratings yet
- Urinary Tract Infections: Dr. Shweta Naik Assistant ProfessorDocument62 pagesUrinary Tract Infections: Dr. Shweta Naik Assistant ProfessorMeenakshisundaram CNo ratings yet
- Urinary Tract Disorders/Infectio NDocument44 pagesUrinary Tract Disorders/Infectio NrintyosoNo ratings yet
- UntitledDocument40 pagesUntitleddNo ratings yet
- ####Bahan Kuliah ISK Blok 23 (Nov 2015)Document32 pages####Bahan Kuliah ISK Blok 23 (Nov 2015)ajengdmrNo ratings yet
- Rinary Ract Nfections: Classification Pathophysiology Risk Factors Clinical Manifestation DiagnosticsDocument27 pagesRinary Ract Nfections: Classification Pathophysiology Risk Factors Clinical Manifestation DiagnosticsDARYmagpantayNo ratings yet
- Urinary Tract InfectionDocument10 pagesUrinary Tract InfectionditaNo ratings yet
- Predisposing FactorsDocument14 pagesPredisposing FactorsThomas GealonNo ratings yet
- Canuuc - Uti May 2017Document31 pagesCanuuc - Uti May 2017Praluki HerliawanNo ratings yet
- 6 UtiDocument18 pages6 UtiMahesh RathnayakeNo ratings yet
- Urinary Tract InfectionsDocument71 pagesUrinary Tract Infectionsdayibon499No ratings yet
- Genitourinary Infections For ClassDocument74 pagesGenitourinary Infections For ClassKashif BurkiNo ratings yet
- Urinary Tract Infection: Akhyar Albaar Haerani RasyidDocument49 pagesUrinary Tract Infection: Akhyar Albaar Haerani Rasyidrolly riksantoNo ratings yet
- Referat - Syifa Firza UtiDocument28 pagesReferat - Syifa Firza Utimiir ikbalNo ratings yet
- 8.urinary Tract Infections-1Document82 pages8.urinary Tract Infections-1fikirjohn8No ratings yet
- Urinary Tract InfectionDocument27 pagesUrinary Tract InfectionNaseem Bin Yoosaf100% (1)
- Elderly Urinary Tract Disorders FixDocument36 pagesElderly Urinary Tract Disorders FixRyan Adi PutraNo ratings yet
- Urinary Tract InfectionDocument9 pagesUrinary Tract InfectionTom Mallinson100% (1)
- Urinary Tract InfectionDocument30 pagesUrinary Tract InfectionLeo Mar MakilanNo ratings yet
- Infeksi Saluran KemihDocument44 pagesInfeksi Saluran KemihAyunda Henna PelalawanNo ratings yet
- (2020) Goldman-Cecil Medicine - Approach To The Patient With Urinary Tract InfectionDocument23 pages(2020) Goldman-Cecil Medicine - Approach To The Patient With Urinary Tract InfectionMiftahurrohmat AlmaasahNo ratings yet
- Urinary Tract InfectionsDocument9 pagesUrinary Tract InfectionsGeethika GummadiNo ratings yet
- Urinary Tract Infection in ChildrenDocument45 pagesUrinary Tract Infection in ChildrenMuhammad HaziqNo ratings yet
- Urinary Tract Infection (Uti) : Yibeltal T (MD)Document24 pagesUrinary Tract Infection (Uti) : Yibeltal T (MD)Lidiya TeshomeNo ratings yet
- UTI in PregnancyDocument33 pagesUTI in Pregnancyyusufkiduchu8No ratings yet
- Urinary System DisordersDocument14 pagesUrinary System DisordersGideon P. CasasNo ratings yet
- Urinary Tract Infection: DR Badriya Al-Mahrouqi 12/11/2017Document51 pagesUrinary Tract Infection: DR Badriya Al-Mahrouqi 12/11/2017NinaNo ratings yet
- Chapter 36 The Urinary System in GynaecologyDocument19 pagesChapter 36 The Urinary System in Gynaecologypmj050gpNo ratings yet
- Kuliah UtiDocument20 pagesKuliah UtiERNINo ratings yet
- Urinary Tract Infection - KULIAH MAHASISWADocument27 pagesUrinary Tract Infection - KULIAH MAHASISWAradhiinathahirNo ratings yet
- Urinary Tract InfectionDocument44 pagesUrinary Tract InfectiongunawanNo ratings yet
- Urinary Tract Infection: DR Humna Najeeb KhanDocument28 pagesUrinary Tract Infection: DR Humna Najeeb KhanSaliha AkramNo ratings yet
- DR Lana Sundac - LGRS Urinary Tract InfectionsDocument4 pagesDR Lana Sundac - LGRS Urinary Tract Infectionsoxford_commaNo ratings yet
- Urinary Tract Infection in Children: DR Nada Qawasmi Alquds Faculty of MedicineDocument25 pagesUrinary Tract Infection in Children: DR Nada Qawasmi Alquds Faculty of Medicineولاء إبراهيمNo ratings yet
- Notes On UtiDocument15 pagesNotes On UtiSaleh Mohammad ShoaibNo ratings yet
- Urinary Tract Infections (UTI)Document58 pagesUrinary Tract Infections (UTI)afdaliaNo ratings yet
- Literature Review On UTIDocument31 pagesLiterature Review On UTINishchal Dhakal0% (1)
- INFEKSI SALURAN KEMIH (ISK) PADA ANAK Blok 14Document26 pagesINFEKSI SALURAN KEMIH (ISK) PADA ANAK Blok 14Siti Shaihany YustikawariNo ratings yet
- Utis in Pregnancy: Rachael Mweigwa NakimuliDocument55 pagesUtis in Pregnancy: Rachael Mweigwa NakimuliRuva Oscass JimmyNo ratings yet
- Uti in PregnancyDocument42 pagesUti in Pregnancydeepak122No ratings yet
- Pathophysiology of Pyelonephritis: How It HappensDocument6 pagesPathophysiology of Pyelonephritis: How It HappensReno Jun NagasanNo ratings yet
- Urinary & Renal Deviations: Edited By: Cynthia Bartlau, MSN, RN, PHNDocument60 pagesUrinary & Renal Deviations: Edited By: Cynthia Bartlau, MSN, RN, PHNmolyebeedNo ratings yet
- UTI and Asymptomatic Bacteriuria TEACHING SLIDESDocument43 pagesUTI and Asymptomatic Bacteriuria TEACHING SLIDESJana DbaibouNo ratings yet
- Urinary Disorders 2Document19 pagesUrinary Disorders 2ula mdiNo ratings yet
- Infectious and Inflammatory Disorders of The Urinary SystemDocument16 pagesInfectious and Inflammatory Disorders of The Urinary SystemBibi Renu100% (1)
- Urinary Tract Infection, (UTI) Is An Infection of One orDocument4 pagesUrinary Tract Infection, (UTI) Is An Infection of One orLorebellNo ratings yet
- Urinary Tract Infection: CC Ricky G. JalecoDocument56 pagesUrinary Tract Infection: CC Ricky G. JalecoRicky JalecoNo ratings yet
- Urinary Tract InfectionDocument50 pagesUrinary Tract InfectionAhmad SobihNo ratings yet
- Obstructive Uropathy: Nitha. K 2 Year MSC NursingDocument67 pagesObstructive Uropathy: Nitha. K 2 Year MSC NursingNITHA KNo ratings yet
- UtiDocument38 pagesUtiAzra AzmunaNo ratings yet
- C5. Renal Disorders FileDocument38 pagesC5. Renal Disorders Filecoco brillqnteNo ratings yet
- UTIDocument46 pagesUTIKiran KommuNo ratings yet
- Urinary Tract Infections in ChildrenDocument2 pagesUrinary Tract Infections in ChildrenKeserovic AdmirNo ratings yet
- Urinary Tract Infection: Tbilisi Referral Hospital, Tbilisi, Georgia Nephrologist Nino MaglakelidzeDocument50 pagesUrinary Tract Infection: Tbilisi Referral Hospital, Tbilisi, Georgia Nephrologist Nino MaglakelidzePayal bhagatNo ratings yet
- Urinary Tract InfectionDocument13 pagesUrinary Tract InfectionMuhamad RockystankiNo ratings yet
- Urinary Tract InfectionDocument50 pagesUrinary Tract Infectionpokhara gharipatanNo ratings yet
- Urinary Tract Infection in Children - Classification, Diagnosis and TreatmentFrom EverandUrinary Tract Infection in Children - Classification, Diagnosis and TreatmentNo ratings yet
- Hematuria, (Blood in Urine) A Simple Guide to The Condition, Related Diseases And Use in Diagnosis of DiseasesFrom EverandHematuria, (Blood in Urine) A Simple Guide to The Condition, Related Diseases And Use in Diagnosis of DiseasesRating: 5 out of 5 stars5/5 (2)
- Abruptio PlasentaDocument17 pagesAbruptio PlasentaJonovSelfNo ratings yet
- Abruptio PlasentaDocument17 pagesAbruptio PlasentaJonovSelfNo ratings yet
- GasterDocument67 pagesGasterteguhNo ratings yet
- Ginjal Patofisiologi 21-2-17Document11 pagesGinjal Patofisiologi 21-2-17JonovSelfNo ratings yet
- Ginjal Patofisiologi 21-2-17Document11 pagesGinjal Patofisiologi 21-2-17JonovSelfNo ratings yet
- Infeksi Organ Reproduksi Pria Dan Wanita: DR Dino Gagah Prihadianto Spog, MkesDocument36 pagesInfeksi Organ Reproduksi Pria Dan Wanita: DR Dino Gagah Prihadianto Spog, MkesJonovSelfNo ratings yet
- Hepatitis Viral AkutDocument50 pagesHepatitis Viral AkutJonovSelfNo ratings yet
- Disain PenelitianDocument38 pagesDisain PenelitianJonovSelfNo ratings yet
- W2 Day 1 Belling The CatDocument23 pagesW2 Day 1 Belling The Catgina domingoNo ratings yet
- ABSTRACT PROF. DR. Dr. ZAKIUDIN MUNASIR SpAKDocument1 pageABSTRACT PROF. DR. Dr. ZAKIUDIN MUNASIR SpAKTimothy Eduard A. SupitNo ratings yet
- CDC - Rabies Around The World - RabiesDocument1 pageCDC - Rabies Around The World - RabieskaminiNo ratings yet
- Practice Test 7. 01.06.2021. 0nlineDocument7 pagesPractice Test 7. 01.06.2021. 0nlineHien NguyenNo ratings yet
- Review in OrthodonticsDocument3 pagesReview in Orthodonticsa3drsabrotNo ratings yet
- Sexual Slang WordsDocument6 pagesSexual Slang WordsXuxu TooNo ratings yet
- Ayurvedic Guidelines To Swineflu or Vatha Sleshmika JwaraDocument4 pagesAyurvedic Guidelines To Swineflu or Vatha Sleshmika JwarasivabharathamurthyNo ratings yet
- Application of Proper DrapingDocument15 pagesApplication of Proper DrapingCharls John Ercillo67% (6)
- Trung tâm Luyện thi Amax - 39 LK 6A Làng Việt Kiều Châu ÂuDocument11 pagesTrung tâm Luyện thi Amax - 39 LK 6A Làng Việt Kiều Châu ÂuKiều Anh NguyễnNo ratings yet
- English Vowel SoundsDocument3 pagesEnglish Vowel SoundsRafil Friasmar100% (1)
- Fed Suit FinalDocument35 pagesFed Suit Finaljerry mcleodNo ratings yet
- Clement-Moore, Rosemary - The Splendor Falls PDFDocument408 pagesClement-Moore, Rosemary - The Splendor Falls PDFLucía BeylesNo ratings yet
- Wilderness Trails Zoo Coloring Activity BookDocument24 pagesWilderness Trails Zoo Coloring Activity BookHolly Crews100% (2)
- À Chaque Jour Suffit Sa PeineDocument35 pagesÀ Chaque Jour Suffit Sa PeineaanurimNo ratings yet
- Momo Avatar CrochetDocument7 pagesMomo Avatar CrochetXochilt SanchezNo ratings yet
- McClain File WMDocument10 pagesMcClain File WMthe kingfishNo ratings yet
- Bdwbu: Bgybv Cövyx CwiwpwzDocument48 pagesBdwbu: Bgybv Cövyx CwiwpwzShariful IslamNo ratings yet
- Diagnosis and Treatment of The Disorders of PigsDocument409 pagesDiagnosis and Treatment of The Disorders of PigsStevanNo ratings yet
- Annotated BibliographyDocument29 pagesAnnotated BibliographyRachel ArnoldNo ratings yet
- H31327 Exam Paper PDFDocument14 pagesH31327 Exam Paper PDFpipoNo ratings yet
- BIO 10 Laboratory ManualDocument55 pagesBIO 10 Laboratory ManualRonneil Bilbao0% (1)
- Sanur WeeklyDocument56 pagesSanur WeeklyGuz NusadaNo ratings yet
- Answers WSKHT Lethal DoseDocument2 pagesAnswers WSKHT Lethal DosejdNo ratings yet
- Big GameDocument75 pagesBig GamekgiyerNo ratings yet