You might also like
- Understanding Laboratory Investigations: A Guide for Nurses, Midwives and Health ProfessionalsFrom EverandUnderstanding Laboratory Investigations: A Guide for Nurses, Midwives and Health ProfessionalsNo ratings yet
- Comprehensive Guide to Managing PCOSDocument48 pagesComprehensive Guide to Managing PCOStata maretha100% (1)
- LymphedemaDocument16 pagesLymphedemaMaulana213No ratings yet
- Metabolism and FertilityDocument15 pagesMetabolism and FertilityGeeklyGamer 02No ratings yet
- Gyne - Feu ReviewerDocument87 pagesGyne - Feu ReviewerKoko RoqueNo ratings yet
- Kidneys BiochemistryDocument53 pagesKidneys BiochemistryMi PatelNo ratings yet
- Pharmacokinetics in a NutshellDocument44 pagesPharmacokinetics in a Nutshellfauziah qurrota a'yuniNo ratings yet
- Summative 2 Renal 2011Document8 pagesSummative 2 Renal 2011Ike Annisa YuwelzaNo ratings yet
- Obs Moses KazevuDocument285 pagesObs Moses KazevuChilufya KalasaNo ratings yet
- ENDOCRINE NURSING-FINAL HDDocument15 pagesENDOCRINE NURSING-FINAL HDJayvee Novenario Casaljay100% (1)
- NCM 102 Care of Mother, Child, and Population Group at Risk or With ProblemsDocument33 pagesNCM 102 Care of Mother, Child, and Population Group at Risk or With ProblemsAyman DaudNo ratings yet
- Farmakokinetika AdmeDocument42 pagesFarmakokinetika AdmeFerda Mahdalena100% (1)
- Hemodiafiltration Kuhlmann PDFDocument31 pagesHemodiafiltration Kuhlmann PDFDavid SantosoNo ratings yet
- Aspek Medis Bedah (Perioperatif) Dan Enteral - Parenteral NutrisiDocument56 pagesAspek Medis Bedah (Perioperatif) Dan Enteral - Parenteral NutrisiJashmine RachlyNo ratings yet
- JMedLife 5 057Document4 pagesJMedLife 5 057Iasmim CabralNo ratings yet
- 2006FallRISE ContentOutlineDocument1 page2006FallRISE ContentOutlinewillygopeNo ratings yet
- Introduction of Pharmacology: Absorption-Distribution-Metabolism-EliminationDocument46 pagesIntroduction of Pharmacology: Absorption-Distribution-Metabolism-Eliminationfransiska labuNo ratings yet
- Ladmer SystemDocument3 pagesLadmer Systemjihan febriyantiNo ratings yet
- Therapeutic Drug Monitoring in The ElderlyDocument3 pagesTherapeutic Drug Monitoring in The ElderlyKristine BaringNo ratings yet
- PEDIA GastroDocument20 pagesPEDIA GastroJoanna :DNo ratings yet
- Anatomy and Physiology Syllabus BreakdownDocument16 pagesAnatomy and Physiology Syllabus BreakdownUjjwal Kumar MauryaNo ratings yet
- Hepatoprotective Activity A Review PharmatutorDocument11 pagesHepatoprotective Activity A Review PharmatutorAbhipsa SinhaNo ratings yet
- Anatomy and Physiology of Female Reprod. System: Menarché Menopause Menstrual Cycle The Ovarian FollicleDocument13 pagesAnatomy and Physiology of Female Reprod. System: Menarché Menopause Menstrual Cycle The Ovarian FollicleKristy Ann Tayo-tubesa ObidosNo ratings yet
- FarmakokinetikaDocument27 pagesFarmakokinetikaRanhie Pen'ned CendhirhieNo ratings yet
- Pharmacology Pharmacokinetics and Pharmacodynamics - PPT - Dr. Maulana Antian Empitu (Airlangga Medical Faculty)Document59 pagesPharmacology Pharmacokinetics and Pharmacodynamics - PPT - Dr. Maulana Antian Empitu (Airlangga Medical Faculty)rizkyyunitaa15No ratings yet
- Carolina MS - Infertility Management in Women With PolycysticDocument8 pagesCarolina MS - Infertility Management in Women With PolycysticCarolina SidabutarNo ratings yet
- Resumen FarmacoDocument9 pagesResumen FarmacoMagali DelvalleNo ratings yet
- Clin PathInterns Review 2019Document33 pagesClin PathInterns Review 2019AmaetenNo ratings yet
- PENYAKIT HATI DAN EMPEDUDocument46 pagesPENYAKIT HATI DAN EMPEDUfannyNo ratings yet
- Drugs and Ans and and Efeects of Mao Inhibitors - Part IIDocument36 pagesDrugs and Ans and and Efeects of Mao Inhibitors - Part IIshikhaNo ratings yet
- Drug Distribution (Kinetika Farmakokinetik)Document14 pagesDrug Distribution (Kinetika Farmakokinetik)princessaurora1998No ratings yet
- Biopharmaceutics Principles in New Drug Delivery SystemsDocument58 pagesBiopharmaceutics Principles in New Drug Delivery SystemsSari RamadhaniNo ratings yet
- Fertility and SubfertilityDocument95 pagesFertility and SubfertilitydidiNo ratings yet
- Obat Pada Bayi Dan AnakDocument47 pagesObat Pada Bayi Dan AnakBrama AtmajaNo ratings yet
- สำเนา Alpelisib PresentDocument74 pagesสำเนา Alpelisib PresentHathaipat OnchamNo ratings yet
- Kuliah 3 Obat-Obat TeratogenikDocument38 pagesKuliah 3 Obat-Obat TeratogenikMuhammad AidilNo ratings yet
- CHRONOPHARMACOLOGYDocument5 pagesCHRONOPHARMACOLOGYalfiya mujawarNo ratings yet
- Maternity Nursing I: Paul Jhon A. Vergara, RNDocument40 pagesMaternity Nursing I: Paul Jhon A. Vergara, RNPaul Jhon VergaraNo ratings yet
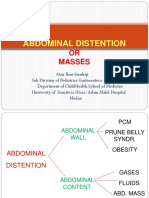
- Abdominal Distention: OR MassesDocument32 pagesAbdominal Distention: OR MassesAbdullah ShiddiqNo ratings yet
- Identify The Above Instrument: - Nasogastric TubeDocument9 pagesIdentify The Above Instrument: - Nasogastric TuberubyNo ratings yet
- Age Drug StudyDocument20 pagesAge Drug StudyLadybelle GototosNo ratings yet
- Ectopic Pregnancy Case Study: Nursing Care Plans and PrognosisDocument21 pagesEctopic Pregnancy Case Study: Nursing Care Plans and PrognosisMardina A AbdulmaulaNo ratings yet
- UCL Formulation of Small Molecules CourseDocument32 pagesUCL Formulation of Small Molecules Coursechegu BusinessNo ratings yet
- NS1 Case PresDocument8 pagesNS1 Case PresjoanaalpayNo ratings yet
- Lecture 1-Overview Blok I.4 (2023)Document42 pagesLecture 1-Overview Blok I.4 (2023)cat shelterNo ratings yet
- Routes of Drug Administration and PharmacokineticsDocument36 pagesRoutes of Drug Administration and PharmacokineticsAbraham ChiuNo ratings yet
- Anovulatory InfertilityDocument57 pagesAnovulatory InfertilityUsha AnengaNo ratings yet
- Pharmacology & Therapeutics Supplements: Ali Raza Chaudary (N67)Document110 pagesPharmacology & Therapeutics Supplements: Ali Raza Chaudary (N67)bajan100% (1)
- CancerDocument10 pagesCancerJoel Andrew Java DagaNo ratings yet
- Intro PhysiologyDocument55 pagesIntro Physiologybrian mburuNo ratings yet
- Pharmacokinetics: Chapter 1: Introduction To PharmacokineticsDocument18 pagesPharmacokinetics: Chapter 1: Introduction To PharmacokineticsTanChantreaNo ratings yet
- Introduction & VomitingDocument47 pagesIntroduction & VomitingSyarifah FauziahNo ratings yet
- Student'S Gynaecology Notes: For Students, by StudentsDocument45 pagesStudent'S Gynaecology Notes: For Students, by StudentsAdli IsmailNo ratings yet
- College of Nursing: Pharmacological ManagementDocument2 pagesCollege of Nursing: Pharmacological ManagementJOHN PEARL FERNANDEZNo ratings yet
- Development of Colon Targeting Drug Delivery System Using Plant PolysaccharideDocument33 pagesDevelopment of Colon Targeting Drug Delivery System Using Plant PolysaccharidePriya SharmaNo ratings yet
- College of Nursing: Cebu Normal UniversityDocument4 pagesCollege of Nursing: Cebu Normal UniversityGwyn RosalesNo ratings yet
- Effect of Metformin On FSH, LH and Prolactin Levels in Patients With Polycystic Ovarian SyndromeDocument4 pagesEffect of Metformin On FSH, LH and Prolactin Levels in Patients With Polycystic Ovarian SyndromeTatjana Nikolić MilivojevićNo ratings yet
- Aeromedical Concerns FOR Therapeutics in Aircrews: 87 A MA A S M A C ADocument30 pagesAeromedical Concerns FOR Therapeutics in Aircrews: 87 A MA A S M A C AAviation MedicineNo ratings yet
- Lecture Pharma Part 1 - 2011-2012Document34 pagesLecture Pharma Part 1 - 2011-2012Harley Justiniani Dela CruzNo ratings yet
- Introduction To Pharmacology: Prof. Johnny S. Bacud JR., RPH, Mspharm CandDocument81 pagesIntroduction To Pharmacology: Prof. Johnny S. Bacud JR., RPH, Mspharm Candlola&losa farhanNo ratings yet
- UPDATED Handout - PHARMA - DR. GRAGEDADocument238 pagesUPDATED Handout - PHARMA - DR. GRAGEDApasabay270No ratings yet
- Control PrenatalDocument29 pagesControl PrenatalClauMcClauNo ratings yet
- LinkDocument1 pageLinkPrayana BanjarnahorNo ratings yet
- Chronic Kidney Disease: Ulysses Rosas May 8, 2012Document19 pagesChronic Kidney Disease: Ulysses Rosas May 8, 2012Mahfud DinNo ratings yet
- Morning Report Ipd Bangsal eDocument11 pagesMorning Report Ipd Bangsal ePrayana BanjarnahorNo ratings yet
- Morning Report Ipd Bangsal eDocument11 pagesMorning Report Ipd Bangsal ePrayana BanjarnahorNo ratings yet
- Dementia Management Strategies Associated With Neuropsychiatric Symptoms ofDocument32 pagesDementia Management Strategies Associated With Neuropsychiatric Symptoms ofPrayana BanjarnahorNo ratings yet
- Tutor Tinjauan PustakaDocument2 pagesTutor Tinjauan PustakaPrayana BanjarnahorNo ratings yet
- Neurobyology Respons Schizophrenia & Other Psychotic DisorderDocument24 pagesNeurobyology Respons Schizophrenia & Other Psychotic DisorderquinnNo ratings yet
- Online Clearance Monitor 4008Document6 pagesOnline Clearance Monitor 4008Dhevi MugNo ratings yet
- Basic pharmacokinetics and its clinical applicationsDocument43 pagesBasic pharmacokinetics and its clinical applicationsPhilippe KinnaerNo ratings yet
- Asthma Bronchial Treatment TheophyllinDocument27 pagesAsthma Bronchial Treatment TheophyllinAci LusianaNo ratings yet
- St. Paul University Philippines: School of Health SciencesDocument8 pagesSt. Paul University Philippines: School of Health SciencesJay Andrea Vea IsraelNo ratings yet
- Pharmacokinetics and safety of single-dose sacubitril/valsartan in healthy Japanese malesDocument10 pagesPharmacokinetics and safety of single-dose sacubitril/valsartan in healthy Japanese malesAntonio SanchezNo ratings yet
- Easterling2018 PDFDocument10 pagesEasterling2018 PDFAhmad SyaukatNo ratings yet
- Pharmacology Exams and NotesDocument17 pagesPharmacology Exams and NotesMrz AlzNo ratings yet
- Dahi̇li̇ye'Detus Sorulari EngDocument83 pagesDahi̇li̇ye'Detus Sorulari EngKhalid ShafiqNo ratings yet
- 2021 重症核心課程CRRT Dose and Prescription-NEW Ver1.0Document63 pages2021 重症核心課程CRRT Dose and Prescription-NEW Ver1.0Andy DazNo ratings yet
- Department of Pharmacy: Course CurriculumDocument14 pagesDepartment of Pharmacy: Course CurriculumNatik Bi IllahNo ratings yet
- Lecture 1 Excrection of Drugs Pharm D 4th Year BPKDocument22 pagesLecture 1 Excrection of Drugs Pharm D 4th Year BPKDaisy Arora KhuranaNo ratings yet
- ASHP Chapter 29 - Medication Dosing in Patients With Renal DysfunctionDocument5 pagesASHP Chapter 29 - Medication Dosing in Patients With Renal DysfunctionTammyNo ratings yet
- Dr. Naitik D Trivedi & Dr. Upama N. Trivedi: Multiple Choice Questions (Analysis and Chemistry)Document35 pagesDr. Naitik D Trivedi & Dr. Upama N. Trivedi: Multiple Choice Questions (Analysis and Chemistry)Seema YadavNo ratings yet
- Creatinine Estimation and Creatinine Clearance TestDocument51 pagesCreatinine Estimation and Creatinine Clearance TestSasimalani SurgunnamNo ratings yet
- Aptitude TestDocument15 pagesAptitude TestGEORGE SARPONGNo ratings yet
- Mobic 15 MG Tablets - Summary of Product Characteristics (SPC)Document11 pagesMobic 15 MG Tablets - Summary of Product Characteristics (SPC)zxvcazcf0% (1)
- Drugs and Pharmaceutical Technology Question BankDocument7 pagesDrugs and Pharmaceutical Technology Question BankVanitha ENo ratings yet
- NPNS QuizDocument2 pagesNPNS QuizAshley TañamorNo ratings yet
- Farmacocinetica LitioDocument20 pagesFarmacocinetica LitioSantiago Arbelaez GuzmánNo ratings yet
- Type of Dialyzers, Clearance and BiocompatibilityDocument53 pagesType of Dialyzers, Clearance and BiocompatibilityDani DanyNo ratings yet
- Non-contacting gas face seals with modified surfacesDocument12 pagesNon-contacting gas face seals with modified surfacesMiguel Angel BeltranNo ratings yet
- Pharmacokinetics and Bioavailability of Florfenicol Following Intravenous, Intramuscular and Oral Administrations in RabbitsDocument10 pagesPharmacokinetics and Bioavailability of Florfenicol Following Intravenous, Intramuscular and Oral Administrations in RabbitsJohanna Valentina López CortesNo ratings yet
- Cbr29 S Pgs53Document8 pagesCbr29 S Pgs53budi_alamsyahNo ratings yet
- Enantiomers Evaluation CetirizineDocument4 pagesEnantiomers Evaluation Cetirizinebebel555No ratings yet
- General Prescribing Guidelines For Geriatric PatientsDocument41 pagesGeneral Prescribing Guidelines For Geriatric PatientsBharath Gowda100% (1)
- 09.30-10.00 Penghitungan KTV PDFDocument15 pages09.30-10.00 Penghitungan KTV PDFaris budionoNo ratings yet
- Sebivo: Name of The MedicineDocument18 pagesSebivo: Name of The MedicineRiez ارسيفدين RibixyNo ratings yet