You might also like
- Notes On Infection PreventionDocument9 pagesNotes On Infection PreventionDipti PunjalNo ratings yet
- Concepts of Infection ControlDocument61 pagesConcepts of Infection Controltummalapalli venkateswara rao100% (1)
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Infection Control PoliciesDocument6 pagesInfection Control PoliciesAlma Moiselle LastimosaNo ratings yet
- Infection Control Nurse: Passbooks Study GuideFrom EverandInfection Control Nurse: Passbooks Study GuideNo ratings yet
- SOP For Spilling ManagementDocument2 pagesSOP For Spilling Managementenumula kumar100% (2)
- Prevention of Needle Stick InjuriesDocument45 pagesPrevention of Needle Stick Injuriesrodcyruskent100% (1)
- Nosocomial InfectionDocument29 pagesNosocomial InfectionNikhil DeurkarNo ratings yet
- Ipsg # 2017 PDFDocument30 pagesIpsg # 2017 PDFDARRYLARANHA100% (1)
- Job Description For Infection Control NurseDocument4 pagesJob Description For Infection Control NurseKeerthi AnbazhaganNo ratings yet
- Infection Control ManualDocument51 pagesInfection Control Manuallimiya varghese100% (1)
- Concepts of Infection Prevention and ControlDocument21 pagesConcepts of Infection Prevention and Controllisalov100% (2)
- Nosocomial InfectionDocument13 pagesNosocomial InfectionwabalyNo ratings yet
- Crash CartDocument55 pagesCrash Carthatem alsrour100% (4)
- Infection ControlDocument13 pagesInfection ControlSheryl Reyes100% (1)
- Surgical Handwashing Resource Material 2023-2024Document9 pagesSurgical Handwashing Resource Material 2023-2024Cherry Louise O. SanvictoresNo ratings yet
- IPSGDocument4 pagesIPSGmohsinaNo ratings yet
- Infection Control ManualDocument205 pagesInfection Control ManualSalah ElbadawyNo ratings yet
- Needle Stick InjuryDocument9 pagesNeedle Stick Injuryinfectioncontrol department100% (1)
- Hospitalist Program Toolkit: A Comprehensive Guide to Implementation of Successful Hospitalist ProgramsFrom EverandHospitalist Program Toolkit: A Comprehensive Guide to Implementation of Successful Hospitalist ProgramsNo ratings yet
- Job Description of Operating Room Nurse in IndiaDocument4 pagesJob Description of Operating Room Nurse in IndiaShine George100% (1)
- Management of Infection Prevention and ControlDocument20 pagesManagement of Infection Prevention and ControlAnna DixonNo ratings yet
- Unit 3-Infection ControlDocument108 pagesUnit 3-Infection Controltau88No ratings yet
- Annex G - Infection Control Annual Plan 2012-13Document7 pagesAnnex G - Infection Control Annual Plan 2012-13Tianti PuadiNo ratings yet
- Pertussis Case Definition and Investigation PresentationDocument62 pagesPertussis Case Definition and Investigation PresentationMuhammad Jahari Supianto100% (1)
- 8A Nosocomial InfectionDocument15 pages8A Nosocomial InfectionSuminaShrestha100% (1)
- ICN Nurse Job ResponsibilitiesDocument2 pagesICN Nurse Job ResponsibilitiesBirupakshya Rout100% (1)
- IPSGDocument29 pagesIPSGShermaida Basirul100% (1)
- Patient SafetyDocument22 pagesPatient SafetyRensy Sabi100% (1)
- Surgical Operation Theater StandardsDocument31 pagesSurgical Operation Theater Standardstummalapalli venkateswara raoNo ratings yet
- Needle RecappingDocument4 pagesNeedle RecappingAyesha Calmerin PenuelaNo ratings yet
- Infection Control ModuleDocument16 pagesInfection Control ModuleKomite PpiNo ratings yet
- Infection Control Program in The HospitalDocument14 pagesInfection Control Program in The HospitalLorelie Asis100% (1)
- DialysisDocument20 pagesDialysisSiwani rai100% (1)
- Infection Control inDocument45 pagesInfection Control inmohdmaghyreh100% (2)
- Infection ControlDocument42 pagesInfection ControlNidhin Thomas67% (3)
- Infection Control Protocols at Travancore Medical College HospitalDocument8 pagesInfection Control Protocols at Travancore Medical College Hospitaltummalapalli venkateswara raoNo ratings yet
- Infection Control: Dr.T.V.Rao MD Professor of MicrobiologyDocument41 pagesInfection Control: Dr.T.V.Rao MD Professor of Microbiologytummalapalli venkateswara rao100% (1)
- Ic ManualDocument416 pagesIc ManualEvangel PaduaNo ratings yet
- In - Patient Service Ward 1Document12 pagesIn - Patient Service Ward 1mitchNo ratings yet
- Respiratory System DisordersDocument9 pagesRespiratory System Disordersasop06No ratings yet
- Infection Prevention BrochureDocument2 pagesInfection Prevention BrochureTeguh Aprian Maulana GultomNo ratings yet
- 25 IcuDocument78 pages25 IcuAloah122346No ratings yet
- IV Therapy ChecklistDocument3 pagesIV Therapy ChecklistJestoni SalvadorNo ratings yet
- Needle Stick Injury & Spill ManagementDocument26 pagesNeedle Stick Injury & Spill Managementprince242653100% (2)
- Nursing Cooperative Wide Infection Control Wound Care Procedures Page 1 of 3Document4 pagesNursing Cooperative Wide Infection Control Wound Care Procedures Page 1 of 3zjaneNo ratings yet
- Seminar On Infetion ControlDocument76 pagesSeminar On Infetion ControlDaisy Vinu0% (1)
- Infection PreventionDocument38 pagesInfection PreventionAmanda ScarletNo ratings yet
- Standard Precaution HandoutDocument3 pagesStandard Precaution Handoutaringkinking100% (1)
- Infection Control ActivitiesDocument3 pagesInfection Control ActivitiesAileen A. MonaresNo ratings yet
- Practical Guidelines Infection Control PDFDocument110 pagesPractical Guidelines Infection Control PDFRao Rizwan Shakoor100% (1)
- MAN-EMPOWERMENT - Strategies For Enhancing Autonomy and Control Over Nursing Practice PDFDocument10 pagesMAN-EMPOWERMENT - Strategies For Enhancing Autonomy and Control Over Nursing Practice PDFfriolan_cacliniNo ratings yet
- Hospital Infection Control ManualDocument32 pagesHospital Infection Control Manualavinash20075% (20)
- INFECTION CONTROL by Sandra WilsonDocument24 pagesINFECTION CONTROL by Sandra WilsonsandraNo ratings yet
- Aseptic TechniqueDocument9 pagesAseptic Techniquebethh_6No ratings yet
- Immunization Manual For Medical and Nursing Students - Final Smaller PDFDocument296 pagesImmunization Manual For Medical and Nursing Students - Final Smaller PDFamit100% (3)
- RNTCPDocument32 pagesRNTCPSuvendu Sekhar PandaNo ratings yet
- IPSGDocument16 pagesIPSGNyimas Milka Ayu NabilaNo ratings yet
- TOEFL Practice QuestionsDocument70 pagesTOEFL Practice QuestionsAlbertoNo ratings yet
- SBI Recording FormsDocument9 pagesSBI Recording FormsElmalyn BernarteNo ratings yet
- Bovi-Shield Gold FP 5 VL5Document2 pagesBovi-Shield Gold FP 5 VL5טורו קוראזוןNo ratings yet
- Care of Child With IncubatorDocument26 pagesCare of Child With IncubatorSabita Paudel100% (2)
- Self-Assessment Colour Review of Small Animal Soft Tissue SurgeryDocument194 pagesSelf-Assessment Colour Review of Small Animal Soft Tissue Surgerymiliindianu100% (3)
- General Properties of Viruses MBDocument15 pagesGeneral Properties of Viruses MBDayana PrasanthNo ratings yet
- First Level Assessment (SAMPLE)Document2 pagesFirst Level Assessment (SAMPLE)Cooby Gempesaw100% (1)
- Immunity and Its TypesDocument3 pagesImmunity and Its TypesBenazir SheikhNo ratings yet
- Infections and ImmunityDocument35 pagesInfections and ImmunityDr. Ashish JawarkarNo ratings yet
- Pathophysiology of HypovolemiaDocument1 pagePathophysiology of HypovolemiaSheana TmplNo ratings yet
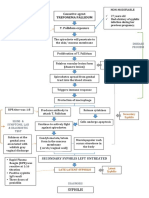
- Path o Physiology of SyphilisDocument1 pagePath o Physiology of Syphilis3S - JOCSON, DENESE NICOLE LEE M.No ratings yet
- Outbreaks: Protecting Americans From Infectious DiseasesDocument116 pagesOutbreaks: Protecting Americans From Infectious DiseasesWatertown Daily Times100% (1)
- Pedia MCUDocument65 pagesPedia MCUfilchibuffNo ratings yet
- Hair CareDocument8 pagesHair CareNeelofur Ibran Ali100% (4)
- Apply Infection Prevention Techniques and Workplace OHSDocument126 pagesApply Infection Prevention Techniques and Workplace OHSTHE TITAN100% (9)
- Know Your Hospital - A Guide To Getting The Best CareDocument9 pagesKnow Your Hospital - A Guide To Getting The Best CareMike PosktovaNo ratings yet
- Bmjopen 2017 July 7 7 Inline Supplementary Material 1 PDFDocument2 pagesBmjopen 2017 July 7 7 Inline Supplementary Material 1 PDFeyabut1No ratings yet
- Week 15 Medical MicrobiologyDocument35 pagesWeek 15 Medical MicrobiologyRuth Ivo Maria TampuboLonNo ratings yet
- PCV 13Document2 pagesPCV 13api-237098034No ratings yet
- Anti-Hemilticos-Parasitologia VeterinariaDocument91 pagesAnti-Hemilticos-Parasitologia VeterinariaTais SenaNo ratings yet
- Safety Action Bundle: Surgical Site Infections (SSI) - ColorectalDocument4 pagesSafety Action Bundle: Surgical Site Infections (SSI) - ColorectalYunita PanjaitanNo ratings yet
- WHO ASEAN Workshop On Priority Actions For Dengue Prevention and CorltrolDocument35 pagesWHO ASEAN Workshop On Priority Actions For Dengue Prevention and CorltrolIvy joan jomocNo ratings yet
- The First Outbreak of Dengue Fever in GreaterDocument14 pagesThe First Outbreak of Dengue Fever in GreaterRizal FahlyNo ratings yet
- Provoking "Eureka" Moments For Effective Infection Control StrategiesDocument3 pagesProvoking "Eureka" Moments For Effective Infection Control StrategiesClaude SUPERNo ratings yet
- Exotic Animals As PetsDocument7 pagesExotic Animals As PetsAndres VazquezNo ratings yet
- Daftar PustakaDocument2 pagesDaftar Pustakacute_chooeyNo ratings yet
- IDAI Online Nov2021-FinalDocument46 pagesIDAI Online Nov2021-FinalEny HardiyantiNo ratings yet
- Introduction To FungiDocument24 pagesIntroduction To FungiNabil holmesNo ratings yet
- Answer Key - Biology EOC Essential Standard Study GuideDocument26 pagesAnswer Key - Biology EOC Essential Standard Study GuideHithe60% (5)
- Diaper Rash: What Is Diaper Rash? What Can I Do If My Baby Gets Diaper Rash?Document2 pagesDiaper Rash: What Is Diaper Rash? What Can I Do If My Baby Gets Diaper Rash?gkNo ratings yet