You might also like
- Leung RS, Katial R, The Diagnosis PDFDocument14 pagesLeung RS, Katial R, The Diagnosis PDF0395No ratings yet
- Piis0095454313001061 PDFDocument8 pagesPiis0095454313001061 PDFAndi WijayaNo ratings yet
- Pharyngitis: Patient Population. ObjectivesDocument10 pagesPharyngitis: Patient Population. ObjectivesjumiNo ratings yet
- Environmental and Non-Infectious Factors in The Aetiology of Pharyngitis (Sore Throat)Document12 pagesEnvironmental and Non-Infectious Factors in The Aetiology of Pharyngitis (Sore Throat)udayana kramasanjayaNo ratings yet
- Smith SR Et Al, Treatment of MildDocument4 pagesSmith SR Et Al, Treatment of Mild0395No ratings yet
- Is The Sex Recession Turning Into A Great Sex DepressionDocument10 pagesIs The Sex Recession Turning Into A Great Sex Depression0395No ratings yet
- Pharyngitis, Diagnosis and Empiric Antibiotic Treatment ConsiderationsDocument7 pagesPharyngitis, Diagnosis and Empiric Antibiotic Treatment ConsiderationsIOSRjournalNo ratings yet
- Firth Et Al-2017-World PsychiatryDocument12 pagesFirth Et Al-2017-World PsychiatryMarco Macavilca CruzNo ratings yet
- Leung RS, Katial R, The Diagnosis PDFDocument14 pagesLeung RS, Katial R, The Diagnosis PDF0395No ratings yet
- Update On Otitis Media - Prevention and Treatment PDFDocument10 pagesUpdate On Otitis Media - Prevention and Treatment PDFangelinefriskaNo ratings yet
- Pharyngitis: Patient Population. ObjectivesDocument10 pagesPharyngitis: Patient Population. ObjectivesjumiNo ratings yet
- Smith SR Et Al, Treatment of MildDocument4 pagesSmith SR Et Al, Treatment of Mild0395No ratings yet
- Piis0095454313001061 PDFDocument8 pagesPiis0095454313001061 PDFAndi WijayaNo ratings yet
- Update On Otitis Media - Prevention and Treatment PDFDocument10 pagesUpdate On Otitis Media - Prevention and Treatment PDFangelinefriskaNo ratings yet
- Causes of The PCG Abnormalities and Onset Juvenile Open-Angle Glaucoma Is Still Not ClearDocument1 pageCauses of The PCG Abnormalities and Onset Juvenile Open-Angle Glaucoma Is Still Not Clear0395No ratings yet
- Otitis Media: Patient Population: ObjectivesDocument12 pagesOtitis Media: Patient Population: Objectivesandi firdha restuwatiNo ratings yet
- Otitis Media Causes & ManagementDocument6 pagesOtitis Media Causes & Management0395No ratings yet
- Daftar Pustaka Penyuluhan YushafiraDocument1 pageDaftar Pustaka Penyuluhan Yushafira0395No ratings yet
- Physical, Biology and Chemical Environment: Its Effect On Ecology and Human HealthDocument24 pagesPhysical, Biology and Chemical Environment: Its Effect On Ecology and Human Health0395No ratings yet
- Otitis Media: Patient Population: ObjectivesDocument12 pagesOtitis Media: Patient Population: Objectivesandi firdha restuwatiNo ratings yet
- Daftar Pustaka Penyuluhan YushafiraDocument1 pageDaftar Pustaka Penyuluhan Yushafira0395No ratings yet
- Sdauijknficskdla Jidalksnd JkcmaszDocument9 pagesSdauijknficskdla Jidalksnd Jkcmasz0395No ratings yet
- Management of Primary Angle-Closure GlaucomaDocument4 pagesManagement of Primary Angle-Closure GlaucomaMerry AndrianyNo ratings yet
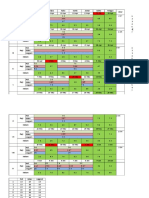
- Jadwal Obgyn NewwDocument4 pagesJadwal Obgyn Neww0395No ratings yet
- Central Serous Chorioretinopathy A Review ofDocument14 pagesCentral Serous Chorioretinopathy A Review of0395No ratings yet
- Chest Radiology For Dummies PDFDocument6 pagesChest Radiology For Dummies PDF0395No ratings yet
- Anatomski Atlas PDFDocument68 pagesAnatomski Atlas PDFIVANANo ratings yet
- DR Gita - Learning StyleDocument34 pagesDR Gita - Learning Style0395No ratings yet
- Path o Physiology o AbDocument8 pagesPath o Physiology o Ab0395No ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Public Health Surveillance-BHWDocument73 pagesPublic Health Surveillance-BHWPaul Angelo E. CalivaNo ratings yet
- Atopic Dermatitis: Skin-Directed Management: Clinical ReportDocument12 pagesAtopic Dermatitis: Skin-Directed Management: Clinical ReportDenia Haritsa AprilianiNo ratings yet
- SGD Case Presentation 10Document26 pagesSGD Case Presentation 10Karen C. Del RosarioNo ratings yet
- Department of Haematology: Test Name Result Unit Bio. Ref. Range MethodDocument4 pagesDepartment of Haematology: Test Name Result Unit Bio. Ref. Range MethodSiddhartha GuptaNo ratings yet
- Necrotizing Facitis ReviewDocument16 pagesNecrotizing Facitis ReviewHadi Firmansyah SidiqNo ratings yet
- Pathogenesis Typhoid Fever PDFDocument7 pagesPathogenesis Typhoid Fever PDFAry Nahdiyani Amalia100% (1)
- 1 Pachet ExpertUltra AngajatiDocument32 pages1 Pachet ExpertUltra Angajaticlaudiu ganeaNo ratings yet
- Biosafety Levels: WWW - Techef.InDocument21 pagesBiosafety Levels: WWW - Techef.InSmk Mahmud KoliNo ratings yet
- Infection & Host ResistanceDocument57 pagesInfection & Host ResistanceBernadette Joyce PascualNo ratings yet
- Bacillus AnthracisDocument44 pagesBacillus AnthracisBalaji KrishnanNo ratings yet
- USMLE IthoughtsDocument1 pageUSMLE Ithoughtsシ DoitrousNo ratings yet
- ImmunityDocument15 pagesImmunitySiyar AhmadNo ratings yet
- Covid-19 Vaccine and The Abortion IssueDocument4 pagesCovid-19 Vaccine and The Abortion IssuerickyNo ratings yet
- Dengue Virus Infection - Prevention and Treatment - UpToDateDocument32 pagesDengue Virus Infection - Prevention and Treatment - UpToDateAnderson SilvaNo ratings yet
- 9-HIV Estimates and Projection For The Year 2021 and 2022Document29 pages9-HIV Estimates and Projection For The Year 2021 and 2022Abel Gebrehiwot AyeleNo ratings yet
- EczemaDocument23 pagesEczemaPn Ziza AzwaNo ratings yet
- Chapter 10 Exam Style QuestionsDocument4 pagesChapter 10 Exam Style QuestionsParth BabardesaiNo ratings yet
- Infection: By: Dr. Abdullah NouhDocument5 pagesInfection: By: Dr. Abdullah NouhMajid Khan100% (1)
- Rheumatoid ArthritisDocument16 pagesRheumatoid Arthritisbudak46No ratings yet
- Non-Hodgkin'S Lymphoma: Oliveros Francis!!!!!!!!!!!!!!!!!Document48 pagesNon-Hodgkin'S Lymphoma: Oliveros Francis!!!!!!!!!!!!!!!!!francis00090No ratings yet
- CDC Modernapfizer EmailsDocument1,433 pagesCDC Modernapfizer EmailsZerohedge JanitorNo ratings yet
- Morgan Mikhails Clinical Anesthesiology 6th Ed 2018 (2114-2211)Document98 pagesMorgan Mikhails Clinical Anesthesiology 6th Ed 2018 (2114-2211)Wiwik SundariNo ratings yet
- OsteomyelitisDocument35 pagesOsteomyelitischinnnababu100% (1)
- c-ANCA ELISADocument2 pagesc-ANCA ELISAYousra ZeidanNo ratings yet
- Patient Case Presentation Rabies 28EM29Document36 pagesPatient Case Presentation Rabies 28EM29Viorica Gavriliță100% (1)
- MCDB 139: Medical Microbiology: Final Exam: Tuesday, June 7 at 7.30 PMDocument2 pagesMCDB 139: Medical Microbiology: Final Exam: Tuesday, June 7 at 7.30 PMAlex AsgariNo ratings yet
- GB Pet Health Certificate - Word FormatDocument9 pagesGB Pet Health Certificate - Word FormatFernanda SoaresNo ratings yet
- 2014-2018 Past Exam Qs + Example Qs For MICR3001Document52 pages2014-2018 Past Exam Qs + Example Qs For MICR3001ekampreetNo ratings yet
- ArticleDocument8 pagesArticleIonescu Raluca VioletaNo ratings yet
- IDSPDocument5 pagesIDSPShreyaswi M KarthikNo ratings yet