You might also like
- Microcytic Hypochromic AnemiasDocument19 pagesMicrocytic Hypochromic Anemiassaket100% (2)
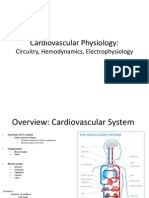
- Cardiovascular Physiology:: Circuitry, Hemodynamics, ElectrophysiologyDocument27 pagesCardiovascular Physiology:: Circuitry, Hemodynamics, Electrophysiologyrsmoney3No ratings yet
- Haemotology Notes Haemotology Notes: Medicine (University of Glasgow) Medicine (University of Glasgow)Document20 pagesHaemotology Notes Haemotology Notes: Medicine (University of Glasgow) Medicine (University of Glasgow)shravaniNo ratings yet
- 01 Bleeding DisordersDocument46 pages01 Bleeding Disordersdee keeNo ratings yet
- A&P 302 Digestive Notes: GI Anatomy, Functions, ProcessesDocument51 pagesA&P 302 Digestive Notes: GI Anatomy, Functions, ProcessesBethanyNo ratings yet
- Porphyrias, Hemoglobinopathies and ThalassemiasDocument11 pagesPorphyrias, Hemoglobinopathies and ThalassemiasGerald John PazNo ratings yet
- RBC Physiology and Blood TypingDocument3 pagesRBC Physiology and Blood TypingGabrielle SerranoNo ratings yet
- Macrocytic AnemiasDocument28 pagesMacrocytic AnemiasDeepankar SrigyanNo ratings yet
- Haematology-Summary My NotesDocument24 pagesHaematology-Summary My NotesToria053No ratings yet
- Skeletal Muscle Contraction MechanismDocument10 pagesSkeletal Muscle Contraction MechanismLiljana StojkovicNo ratings yet
- Chapter 11: Blood 11.1 Functions of Blood: - 91% Water - 7% Proteins (Dissolved)Document3 pagesChapter 11: Blood 11.1 Functions of Blood: - 91% Water - 7% Proteins (Dissolved)Jennifer HerediaNo ratings yet
- LSM3212 - Lecture 2-4 BloodDocument59 pagesLSM3212 - Lecture 2-4 BloodAbraham KangNo ratings yet
- Plasma Physiology (1-2020) by DR Khaled A AbulfadleDocument9 pagesPlasma Physiology (1-2020) by DR Khaled A AbulfadleUzama Binu AliNo ratings yet
- Anatomy & Physiology (Chapter 18 - Urinary System)Document12 pagesAnatomy & Physiology (Chapter 18 - Urinary System)Eliezer NuenayNo ratings yet
- RBC Formation, Anemia, WBC FunctionDocument28 pagesRBC Formation, Anemia, WBC FunctionlifecostNo ratings yet
- HemostasisDocument48 pagesHemostasissianturisuryaNo ratings yet
- Surgical Conditions of Pleura: Kibrom Gebreselassie, MD, FCS-ECSA Cardiovascular and Thoracic SurgeonDocument63 pagesSurgical Conditions of Pleura: Kibrom Gebreselassie, MD, FCS-ECSA Cardiovascular and Thoracic SurgeonVincent SerNo ratings yet
- Lecture 3. Bleeding Disorders Part 1Document31 pagesLecture 3. Bleeding Disorders Part 1Kekelwa Mutumwenu Snr100% (1)
- Hematologic DisordersDocument197 pagesHematologic DisordersDanica Mae BianitoNo ratings yet
- Histology of Male Reproductive SystemDocument3 pagesHistology of Male Reproductive SystemSanna Asila AkramNo ratings yet
- 9 ThalamusDocument10 pages9 ThalamusZoya MoraniNo ratings yet
- 1.02 Physiology Trans - Muscle PhysiologyDocument10 pages1.02 Physiology Trans - Muscle PhysiologyMineTagraNo ratings yet
- A&P 302 - Respiratory NotesDocument31 pagesA&P 302 - Respiratory NotesBethanyNo ratings yet
- Megaloblastic and Other Macrocytic Anaemia: Dr. Nilukshi Perera Consultant HaematologistDocument58 pagesMegaloblastic and Other Macrocytic Anaemia: Dr. Nilukshi Perera Consultant HaematologistThaveeshaLindsayWhiteNo ratings yet
- 4 Apr - Bleeding DisordersDocument50 pages4 Apr - Bleeding DisordersAhmed SarfarazNo ratings yet
- Heart Muscles, Valves & Blood Vessels (I)Document31 pagesHeart Muscles, Valves & Blood Vessels (I)Hussain GauharNo ratings yet
- Blood Components Where Do They Come From?: Introduction To HaematologyDocument11 pagesBlood Components Where Do They Come From?: Introduction To Haematologydorsa koraeiNo ratings yet
- Blood Cells, Immunity and Blood ClottingDocument65 pagesBlood Cells, Immunity and Blood Clottingmunaamuummee100% (1)
- of Cell Adhesion and Cell JunctionsDocument50 pagesof Cell Adhesion and Cell Junctionsayad ghawiNo ratings yet
- ANPH-M2-CU8. The HeartDocument20 pagesANPH-M2-CU8. The HeartMary Grace MapulaNo ratings yet
- Essentials of Anatomy & Physiology: The SensesDocument22 pagesEssentials of Anatomy & Physiology: The SensesKBS100% (1)
- Acute Leukemias: Causes, Types, Symptoms and TreatmentDocument60 pagesAcute Leukemias: Causes, Types, Symptoms and TreatmentThaveeshaLindsayWhite100% (1)
- 1st Lec On Heart Physiology by Dr. RoomiDocument13 pages1st Lec On Heart Physiology by Dr. RoomiMudassar Roomi100% (1)
- Anemia-Dr Moses KazevuDocument86 pagesAnemia-Dr Moses KazevuMoses Jr KazevuNo ratings yet
- Blood 12-6-2018Document42 pagesBlood 12-6-2018Noor Fatima100% (1)
- Introduction To Cell PhysiologyDocument149 pagesIntroduction To Cell PhysiologyAlysaNo ratings yet
- Physiology of The Cardiovascular System-CVSDocument56 pagesPhysiology of The Cardiovascular System-CVSAmanuel MaruNo ratings yet
- HB Synthesis, Degradation, Jaundice, Iron Metabolism by Dr. RoomiDocument23 pagesHB Synthesis, Degradation, Jaundice, Iron Metabolism by Dr. RoomiMudassar Roomi100% (1)
- Patho Physiology Lecture13Document10 pagesPatho Physiology Lecture13Manar AlzobiNo ratings yet
- 3rd Lecture On Skeletal Muscle Physiology by DR - RoomiDocument21 pages3rd Lecture On Skeletal Muscle Physiology by DR - RoomiMudassar Roomi67% (3)
- Kidney Physiology (Q & A)Document28 pagesKidney Physiology (Q & A)ramadan100% (1)
- 1.cardiac Muscle The Heart As A Pump and Function of The Heart Valves 2022Document73 pages1.cardiac Muscle The Heart As A Pump and Function of The Heart Valves 2022Sezanur Taalaibek kyzyNo ratings yet
- (PHYSIO B) 1.2 Renal Physio Pt. 3Document8 pages(PHYSIO B) 1.2 Renal Physio Pt. 3miguel cuevasNo ratings yet
- Vascular System Vascular Structure and FunctionDocument8 pagesVascular System Vascular Structure and FunctionEriq BaldovinoNo ratings yet
- ME114-Benign Disorders of White Blood CellsDocument45 pagesME114-Benign Disorders of White Blood CellsqianyuNo ratings yet
- 2 Medicine HematologyDocument78 pages2 Medicine HematologyAmitNo ratings yet
- A&P 302 Renal Lecture NotesDocument58 pagesA&P 302 Renal Lecture NotesBethanyNo ratings yet
- L1 Composition and Function of BloodDocument20 pagesL1 Composition and Function of BloodManila BhatiaNo ratings yet
- Embryo NotesDocument52 pagesEmbryo NotesSharona Avgush100% (1)
- BLOOD CELL PRODUCTION AND FUNCTIONSDocument59 pagesBLOOD CELL PRODUCTION AND FUNCTIONSMarieana Gomez100% (1)
- 18 Characteristics of Leukemias Lymphomas and MyelomasDocument9 pages18 Characteristics of Leukemias Lymphomas and MyelomasDaphne HernaezNo ratings yet
- Blood ComponentsDocument17 pagesBlood ComponentsJohnSmithNo ratings yet
- Table of Leukemias and LymphomasDocument7 pagesTable of Leukemias and LymphomasRhenjay Ferrer Lagoy100% (1)
- Welcome To Seminar: Dr. Aysha Sabiha Dr. Maimuna Sayeed Dr. Sharmin Akter Luna Residents (Phase-A)Document124 pagesWelcome To Seminar: Dr. Aysha Sabiha Dr. Maimuna Sayeed Dr. Sharmin Akter Luna Residents (Phase-A)interna MANADONo ratings yet
- Lipoprotein Disorders 2Document33 pagesLipoprotein Disorders 2Bolabo BenivoNo ratings yet
- Biology Immunology Course HighlightsDocument34 pagesBiology Immunology Course HighlightsAhmed Asaad Majid Al Mousawi100% (1)
- Secretory Functions of GITDocument24 pagesSecretory Functions of GITDr.Nusrat TariqNo ratings yet
- Anemia in ChildrenDocument67 pagesAnemia in ChildrenDenny BimatamaNo ratings yet
- Red Blood Cells and Anemias: Jonathan Ben-Ezra, M.DDocument33 pagesRed Blood Cells and Anemias: Jonathan Ben-Ezra, M.Diloveit52252No ratings yet
- Anemia in Childhood, Physiopathology and Clinical Findings Bleeding Tests in ChildhoodDocument76 pagesAnemia in Childhood, Physiopathology and Clinical Findings Bleeding Tests in Childhoodmohammed barwaryNo ratings yet
- Rajeev Sir.Document1 pageRajeev Sir.rohitNo ratings yet
- Mullerian Duct Abnormalities, Hirsutism, Bacterial Vaginosis & IUCDsDocument4 pagesMullerian Duct Abnormalities, Hirsutism, Bacterial Vaginosis & IUCDsrohitNo ratings yet
- Brochure CWMUN Emirates 2023 ROWDocument12 pagesBrochure CWMUN Emirates 2023 ROWrohitNo ratings yet
- DME PG MDMS Course Second Round Allotment Result 2022Document34 pagesDME PG MDMS Course Second Round Allotment Result 2022rohitNo ratings yet
- Diagnostic Imaging Approach To A Supratentorial SOLDocument27 pagesDiagnostic Imaging Approach To A Supratentorial SOLAnonymous ql5nwYKVgaNo ratings yet
- AlkalosisAcidosis CasesDocument5 pagesAlkalosisAcidosis CasesrohitNo ratings yet
- Buergers Disease, Thoracic Outlet Syndrome & AneurysmDocument21 pagesBuergers Disease, Thoracic Outlet Syndrome & AneurysmrohitNo ratings yet
- Classification and Management of Wound, Principle of Wound Healing, Haemorrhage and Bleeding ControlDocument39 pagesClassification and Management of Wound, Principle of Wound Healing, Haemorrhage and Bleeding ControlrohitNo ratings yet
- Anal CanerDocument9 pagesAnal CanerrohitNo ratings yet
- Combined Questions FinalDocument17 pagesCombined Questions FinalrohitNo ratings yet
- Im CaseDocument7 pagesIm CaserohitNo ratings yet
- Inguinal Hernias CmeDocument64 pagesInguinal Hernias CmerohitNo ratings yet
- 4th 11th: Age 60-70yrsDocument33 pages4th 11th: Age 60-70yrsrohitNo ratings yet
- Q&A 3ednDocument15 pagesQ&A 3ednrohitNo ratings yet
- Head & Neck1.jpgDocument2 pagesHead & Neck1.jpgrohitNo ratings yet
- Pru RitisDocument40 pagesPru RitisrohitNo ratings yet
- Assessing A CXRDocument2 pagesAssessing A CXRrohitNo ratings yet
- Buergers Disease, Thoracic Outlet Syndrome & AneurysmDocument21 pagesBuergers Disease, Thoracic Outlet Syndrome & AneurysmrohitNo ratings yet
- Intestinal Obstruction ChikaDocument45 pagesIntestinal Obstruction ChikarohitNo ratings yet
- Vascular System PathologyDocument63 pagesVascular System PathologyrohitNo ratings yet
- Kidney and Testicular CancerDocument18 pagesKidney and Testicular CancerrohitNo ratings yet
- Central Venous Catheters: Iv Terapy &Document71 pagesCentral Venous Catheters: Iv Terapy &Florence Liem0% (1)
- MoneyDocument29 pagesMoneyrohitNo ratings yet
- Raksha Yadav B.SC Nursing 2 Year Aiims, JodhpurDocument22 pagesRaksha Yadav B.SC Nursing 2 Year Aiims, JodhpurrohitNo ratings yet
- HematuriaDocument14 pagesHematuriarohitNo ratings yet
- Nxiety Isorders: P - P E M S EDocument11 pagesNxiety Isorders: P - P E M S ErohitNo ratings yet
- For More Details Please Visit Our WebsiteDocument9 pagesFor More Details Please Visit Our WebsiterohitNo ratings yet
- Distribution of Body FluidsDocument41 pagesDistribution of Body FluidsrohitNo ratings yet
- Renal Calculi: /Stone/NephrolithiasisDocument25 pagesRenal Calculi: /Stone/NephrolithiasisrohitNo ratings yet
- Renal Calculi: Urolithiasis, Nephrolithiasis, Renal StoneDocument18 pagesRenal Calculi: Urolithiasis, Nephrolithiasis, Renal StonerohitNo ratings yet
- Sample PET Report 1Document2 pagesSample PET Report 1Samir S. ShahNo ratings yet
- Thread Lift in Breast Ptosis: CorrespondenceDocument3 pagesThread Lift in Breast Ptosis: CorrespondenceElaine MedeirosNo ratings yet
- Siemens Acuson Sc2000 Interventional FlyerDocument6 pagesSiemens Acuson Sc2000 Interventional Flyerbashir019No ratings yet
- DR Loai Saadah CV - JustDocument10 pagesDR Loai Saadah CV - Justapi-370870321No ratings yet
- Q& A PharmacologyDocument17 pagesQ& A PharmacologyFilipino Nurses CentralNo ratings yet
- Unit 304 Prepare and Maintain Environment, Instruments and Equipment For Clinical Dental ProceduresDocument5 pagesUnit 304 Prepare and Maintain Environment, Instruments and Equipment For Clinical Dental Proceduresjolene johnstonNo ratings yet
- ACOG Practice Bulletin No163Document15 pagesACOG Practice Bulletin No163Marco DiestraNo ratings yet
- Rohini Shakya: Personal StatementDocument3 pagesRohini Shakya: Personal Statementapi-427643823No ratings yet
- Is Lab P4 - Serologic Tests For SyphilisDocument4 pagesIs Lab P4 - Serologic Tests For SyphilisDanielle Anne LambanNo ratings yet
- Edible VaccinesDocument17 pagesEdible Vaccinesvishnupushpita100% (1)
- Adelax: Only For The Use of Medical ProfessionalsDocument2 pagesAdelax: Only For The Use of Medical Professionalsparthibanemails5779No ratings yet
- Nursing Care of Client During Labor and Delivery 1Document8 pagesNursing Care of Client During Labor and Delivery 1Arcel SasaluyaNo ratings yet
- Nursing Care Plan for Neonatal SepsisDocument2 pagesNursing Care Plan for Neonatal SepsisPanJan BalNo ratings yet
- NMC RegistrationDocument19 pagesNMC RegistrationcissylNo ratings yet
- Medicalization: History and Theory HSSC 532 /HIST 534/SOCI 513Document4 pagesMedicalization: History and Theory HSSC 532 /HIST 534/SOCI 513sofroniscoNo ratings yet
- Cara PenyuntikanDocument2 pagesCara Penyuntikankhaira_nNo ratings yet
- 17.ophthalmology Final PDFDocument120 pages17.ophthalmology Final PDFluckyNo ratings yet
- RD Symptoms Causes TreatmentsDocument2 pagesRD Symptoms Causes Treatmentswieka mawieNo ratings yet
- 60-Day Limited Period For Changes To Existing Elections Under The Federal Flexible Spending Account Program FSAFEDSDocument4 pages60-Day Limited Period For Changes To Existing Elections Under The Federal Flexible Spending Account Program FSAFEDSFedSmith Inc.100% (1)
- Sample Report Blood Group SubDocument1 pageSample Report Blood Group SubNarayan ChauhanNo ratings yet
- Bayer Breeze2 User ManualDocument55 pagesBayer Breeze2 User ManualYvan Jacen ErnacioNo ratings yet
- Arnold-Chiari Malformations Types PDFDocument3 pagesArnold-Chiari Malformations Types PDFsridharNo ratings yet
- Respiratory SystemDocument15 pagesRespiratory SystemMonicaNo ratings yet
- Tracheostomy 4Document5 pagesTracheostomy 4rizwanNo ratings yet
- Metformin Medication Guide - Uses, Side Effects, DosageDocument5 pagesMetformin Medication Guide - Uses, Side Effects, DosageAgronaSlaughterNo ratings yet
- Courses: Experience Dental Professionals Around The WorldDocument2 pagesCourses: Experience Dental Professionals Around The WorldRadoslav AsparuhovNo ratings yet
- Feline Injection-Site SarcomaDocument8 pagesFeline Injection-Site SarcomaMr. questionNo ratings yet
- Proton Beam TherapyDocument34 pagesProton Beam Therapyyee siew huatNo ratings yet
- Medical Examination Before Appointment Part 1 - Candidate A2Document6 pagesMedical Examination Before Appointment Part 1 - Candidate A2Andreea LarisaNo ratings yet
- Postgrad HD Non Nephro POD - Registration Form WebinarDocument1 pagePostgrad HD Non Nephro POD - Registration Form Webinarmigz516No ratings yet