You might also like
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Hepatomegaly: Clinical ApproachDocument22 pagesHepatomegaly: Clinical ApproachPooja ShashidharanNo ratings yet
- Liver Cirrhosis Nursing Care PlansDocument17 pagesLiver Cirrhosis Nursing Care Plansmarsan12No ratings yet
- Types of Reconstructive & Cosmetic SurgeryDocument28 pagesTypes of Reconstructive & Cosmetic SurgerySimon JosanNo ratings yet
- Intercostal DrainDocument44 pagesIntercostal Drainvamshidh100% (1)
- Upper Gastrointestinal BleedingDocument24 pagesUpper Gastrointestinal BleedingDr.Sathaporn Kunnathum100% (1)
- Standing Order-Diarrhea DraftDocument1 pageStanding Order-Diarrhea DraftKatelyn Brissey50% (2)
- Revised Case Study Umbilical HerniaDocument14 pagesRevised Case Study Umbilical HerniaLance Angelo Bernandino100% (1)
- 14.malabsorption SyndromesDocument5 pages14.malabsorption SyndromesPriyaNo ratings yet
- Esophageal Stricture and ObstructionDocument11 pagesEsophageal Stricture and ObstructionBibi Renu100% (6)
- Nursing Management: OF ArteriosclerosisDocument6 pagesNursing Management: OF ArteriosclerosisANCHAL SHARMANo ratings yet
- CystitisDocument24 pagesCystitisTaufik Ramadhan BiyaNo ratings yet
- Anatomy and Physiology BPH!Document1 pageAnatomy and Physiology BPH!Christian BuenaNo ratings yet
- Organophosphate PoisoningDocument40 pagesOrganophosphate PoisoningMadhu Sudhan PandeyaNo ratings yet
- Anatomy and Physiology of GallbladderDocument15 pagesAnatomy and Physiology of GallbladderIkea Balhon100% (1)
- HIATAL HERNIA PPT Final PDFDocument49 pagesHIATAL HERNIA PPT Final PDFregysujit60% (5)
- Chronic Renal FailureDocument54 pagesChronic Renal FailureAkia Cayasan BayaNo ratings yet
- Hepatic EncephalopathyDocument3 pagesHepatic EncephalopathySuhas KandeNo ratings yet
- Cirrhosis of LiverDocument22 pagesCirrhosis of LiverKrini Tandel50% (2)
- Gastric Cancer: Calag, Prescilla Tavas, Charme FayeDocument20 pagesGastric Cancer: Calag, Prescilla Tavas, Charme FayeDareRaymond0% (1)
- Case of Obstructive JaundiceDocument23 pagesCase of Obstructive JaundiceAjay Agrawal100% (1)
- GERDDocument32 pagesGERDlumina.sNo ratings yet
- HYPERTENSIONDocument11 pagesHYPERTENSIONGargiNo ratings yet
- Hernia: Done by D1 GroupDocument47 pagesHernia: Done by D1 Groupanindyadputri100% (1)
- ABG InterpretationDocument23 pagesABG Interpretationprateekbatra0% (1)
- Gastroesophageal Reflux Disease (GERD)Document23 pagesGastroesophageal Reflux Disease (GERD)Alexis TrinidadNo ratings yet
- Renal AbscessDocument13 pagesRenal Abscessawalsher100% (1)
- Nursing Care PlanDocument6 pagesNursing Care Plankreny1050% (2)
- Careplan Medication ListDocument17 pagesCareplan Medication ListGiorgia ScorsoneNo ratings yet
- Esophageal ObstructionDocument18 pagesEsophageal ObstructionArun Murali50% (2)
- Chronic Renal FailureDocument46 pagesChronic Renal Failurestepharry08100% (1)
- Anatomy and Physiology-Liver CirrhosisDocument2 pagesAnatomy and Physiology-Liver CirrhosisHilmi Ramos100% (3)
- Acid Peptic DiseaseDocument19 pagesAcid Peptic DiseaseKasuganti koteshwar rao100% (2)
- Acute PancreatitisDocument7 pagesAcute PancreatitisVytheeshwaran Vedagiri100% (9)
- PP Insect Bite 2007 (Print)Document16 pagesPP Insect Bite 2007 (Print)Ali RumiNo ratings yet
- Westfort College of Nursing Osce-Cardiopulmonary ResuscitationDocument1 pageWestfort College of Nursing Osce-Cardiopulmonary Resuscitationvishnu100% (1)
- Anatomy and Physiology of Peptic UlcerDocument16 pagesAnatomy and Physiology of Peptic UlcerDrNarayan KR100% (8)
- Liver TransplantationDocument22 pagesLiver Transplantationrajan kumar100% (6)
- 3 - Diagnosis of PregnancyDocument5 pages3 - Diagnosis of PregnancyM7 AlfatihNo ratings yet
- Chronic Liver DiseaseDocument30 pagesChronic Liver Diseaseprajwal86% (7)
- Nursing Care Plan For Diabetes Mellitus Diabetic KetoacidosisDocument17 pagesNursing Care Plan For Diabetes Mellitus Diabetic KetoacidosisJordz Placi100% (2)
- Digital Rectal ExaminationDocument17 pagesDigital Rectal Examinationyulianpatriawan100% (2)
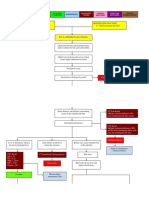
- Case Presentation On Rheumatoid ArthritisDocument36 pagesCase Presentation On Rheumatoid ArthritisGADDAM TEJASWINI50% (2)
- Liver AbscessDocument15 pagesLiver AbscessAli Aborges Jr.No ratings yet
- Chronic Liver DiseaseDocument12 pagesChronic Liver DiseaseamitNo ratings yet
- Case Study On Gastric Outlet ObstructionDocument37 pagesCase Study On Gastric Outlet ObstructionJunayed Safar Mahmud100% (4)
- Antenatal History FormatDocument8 pagesAntenatal History FormatAnnapurna DangetiNo ratings yet
- Swine FluDocument4 pagesSwine FluNader Smadi100% (2)
- Swaminathan - Pathology & Genetics For Nurses 3EDocument1 pageSwaminathan - Pathology & Genetics For Nurses 3EAYOMIDE SILEOLA OLADOSU50% (2)
- Emergency Trolly Lecture 2Document28 pagesEmergency Trolly Lecture 2Eggy Pascual100% (1)
- Nursing Management of Patient With Mechanical VentilationDocument77 pagesNursing Management of Patient With Mechanical Ventilationrojina poudel0% (1)
- 13th & 14th WK - Oxygen Therapy With VideoDocument89 pages13th & 14th WK - Oxygen Therapy With VideoJesus Mario Lopez100% (1)
- 8 Liver Cirrhosis Nursing Care PlansDocument4 pages8 Liver Cirrhosis Nursing Care PlansAngie MandeoyaNo ratings yet
- History of MSNDocument20 pagesHistory of MSNSyamVRNo ratings yet
- Pre - Operative and Post Operative CareDocument52 pagesPre - Operative and Post Operative CareChonnetteAshlynKingNo ratings yet
- PeritonitisDocument22 pagesPeritonitisBobby Faisyal Rakhman100% (1)
- NCP Liver CirrhosisDocument7 pagesNCP Liver CirrhosisIris Jimenez-BuanNo ratings yet
- Intra Aortic Balloon PumpDocument51 pagesIntra Aortic Balloon PumpDeeksha Rajput100% (2)
- Long Case JaundiceDocument5 pagesLong Case JaundiceNadia SalwaniNo ratings yet
- Jaundice MasterDocument76 pagesJaundice MasterSuresh Kubavat100% (3)
- Atlas of Anatomic Hepatic Resection For Hepatocellular CarcinomaDocument339 pagesAtlas of Anatomic Hepatic Resection For Hepatocellular CarcinomaValean Dan100% (1)
- Pathophysiology - Obstructive JaundiceDocument3 pagesPathophysiology - Obstructive JaundiceAbigail Lonogan0% (1)
- Cholecystitis Pathophysiology Schematic DiagramDocument2 pagesCholecystitis Pathophysiology Schematic DiagramChristyl CalizoNo ratings yet
- Jaundie 2Document25 pagesJaundie 2Nambuye Midyero AhmedNo ratings yet
- MRI Protokol Review Adi WS QCDocument150 pagesMRI Protokol Review Adi WS QChadiNo ratings yet
- Management of Obstructive Jaundice Exper PDFDocument3 pagesManagement of Obstructive Jaundice Exper PDFgustianto hutama pNo ratings yet
- Cholecystitis IntroductionDocument4 pagesCholecystitis IntroductionJechelle Ann Pabustan Martin-BoniquitNo ratings yet
- Jurnal MRCPDocument18 pagesJurnal MRCPMaharani Eka SaputriNo ratings yet
- Judul PutriDocument27 pagesJudul PutriFaizah Betty RahayuningsihNo ratings yet
- 3d NLS Study of Gall Bladder and Gall Ducts ConcretionsDocument3 pages3d NLS Study of Gall Bladder and Gall Ducts ConcretionstestnationNo ratings yet
- Clinical Case On JaundiceDocument43 pagesClinical Case On JaundicePro fatherNo ratings yet
- Contractility IndexDocument4 pagesContractility IndexisnainiNo ratings yet
- Kyamch January 2020 2ndDocument6 pagesKyamch January 2020 2ndDr. Fardil HossainNo ratings yet
- Cholestasis PPT - PPT FixDocument31 pagesCholestasis PPT - PPT FixmeisygraniaNo ratings yet
- Fluids Foods Did You Urinate?: Bladder DiaryDocument1 pageFluids Foods Did You Urinate?: Bladder DiaryAnika TasnimNo ratings yet
- Cholangiopancreatography (MRCP) Coronal Pada Sekuen T2 FrfseDocument7 pagesCholangiopancreatography (MRCP) Coronal Pada Sekuen T2 FrfseAditya MegaNo ratings yet
- Acute CholecystitisDocument3 pagesAcute CholecystitisًNo ratings yet
- Congenital Anomalies and Variations of The Bile and Pancreatic Ducts - Magnetic Resonance Cholangiopancreatography Findings, Epidemiology and Clinical SignificanceDocument19 pagesCongenital Anomalies and Variations of The Bile and Pancreatic Ducts - Magnetic Resonance Cholangiopancreatography Findings, Epidemiology and Clinical SignificanceRoberto HernandezNo ratings yet
- CholelithiasisDocument6 pagesCholelithiasisLara GatbontonNo ratings yet
- CholelithiasisDocument65 pagesCholelithiasisGAURAV0% (1)
- Hepatobiliary SystemDocument18 pagesHepatobiliary SystemBinita ShresthaNo ratings yet
- Liver: Anatomy & FunctionsDocument18 pagesLiver: Anatomy & FunctionsDR NARENDRANo ratings yet
- Alt Ast Alp GGT Pada Liver DiseaseDocument5 pagesAlt Ast Alp GGT Pada Liver DiseaseNararto PrijogoNo ratings yet
- Alcoholic Liver DiseaseDocument3 pagesAlcoholic Liver DiseaseEglNo ratings yet
- Acute Biliary PancreatitisDocument12 pagesAcute Biliary Pancreatitisfiareza dilagaNo ratings yet
- Cholelithiasis: Group MembersDocument12 pagesCholelithiasis: Group MembersShiela GutierrezNo ratings yet
- Gall Bladder and Bile DuctDocument18 pagesGall Bladder and Bile DuctClint MorrisonNo ratings yet
- Gallstone DiseaseDocument14 pagesGallstone DiseasePrincess Meinny JeanNo ratings yet
- Abnormal LFTsDocument2 pagesAbnormal LFTsRenu RosyNo ratings yet
- Cholestasis: View Full-Size ImageDocument15 pagesCholestasis: View Full-Size Imagearambakkam100% (2)