You might also like
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Revision For The First 1 English 8Document6 pagesRevision For The First 1 English 8hiidaxneee urrrmNo ratings yet
- Module Letter 1Document2 pagesModule Letter 1eeroleNo ratings yet
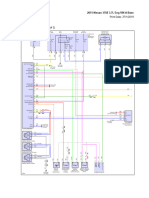
- 2015 Nissan 370Z 3.7L Eng VIN A BaseDocument69 pages2015 Nissan 370Z 3.7L Eng VIN A BaseData TécnicaNo ratings yet
- Medical BiotechnologyDocument4 pagesMedical Biotechnologyعمر بن عليNo ratings yet
- Ford6000cd Rear ConnectorDocument2 pagesFord6000cd Rear ConnectorAnonymous WcYW9AeNo ratings yet
- MCQ Unit 3Document15 pagesMCQ Unit 3gaur1234No ratings yet
- Material Control Procedure - TemplateDocument5 pagesMaterial Control Procedure - TemplateHernandito Rahmat KusumaNo ratings yet
- Fundamental and Technical Analysis of Iron and Steel SIP PROJECTDocument34 pagesFundamental and Technical Analysis of Iron and Steel SIP PROJECThaveuever910No ratings yet
- CON21 6th EditionDocument65 pagesCON21 6th EditionDavid WeeNo ratings yet
- Alien Magic - William Hamilton IIIDocument179 pagesAlien Magic - William Hamilton IIICarlos Rodriguez100% (7)
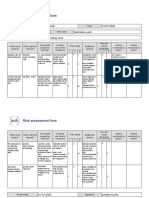
- Risk Assessment Project Iosh - MsDocument2 pagesRisk Assessment Project Iosh - MsSanjeev Kumar75% (32)
- Psychological Factors Influencing Technology Adoption A Case S - 2021 - TechnovDocument17 pagesPsychological Factors Influencing Technology Adoption A Case S - 2021 - Technov6helmi6nauval6No ratings yet
- Portable Load Banks: CressallDocument1 pagePortable Load Banks: CressallYashveer26No ratings yet
- Mice and Men Naturalism Web SiteDocument10 pagesMice and Men Naturalism Web SitedrooolNo ratings yet
- Brochure - Citadines Flatiron Phnom Penh - EnglishDocument4 pagesBrochure - Citadines Flatiron Phnom Penh - EnglishTix VirakNo ratings yet
- 120Document349 pages120xdyj2005No ratings yet
- hw10 PDFDocument10 pageshw10 PDFTahok24No ratings yet
- 02 Unit I Environmental Studies-A Multidisciplinary Subject 14-01-2022Document69 pages02 Unit I Environmental Studies-A Multidisciplinary Subject 14-01-2022doramonbhaiyaNo ratings yet
- GPT Protocol - Trypcase Soy AgarDocument8 pagesGPT Protocol - Trypcase Soy AgarmailboxofmurliNo ratings yet
- Asms 02 0033Document6 pagesAsms 02 0033Delfia AkiharyNo ratings yet
- Commissioning/Troubleshooting: Check List: C B A Yellow Grey Black TBPDocument2 pagesCommissioning/Troubleshooting: Check List: C B A Yellow Grey Black TBPmohamedNo ratings yet
- A Bilateral Subdural Hematoma Case Report 2165 7548.1000112 PDFDocument2 pagesA Bilateral Subdural Hematoma Case Report 2165 7548.1000112 PDFPutra GagahNo ratings yet
- Paper 1Document4 pagesPaper 1asa.henfield2No ratings yet
- Biology F4 Review Summary NoteDocument117 pagesBiology F4 Review Summary NoteSocdal AbdiNo ratings yet
- 5-2 Sem2 Phys ExamDocument7 pages5-2 Sem2 Phys ExamNayLinNo ratings yet
- Forest Flower October 2018Document24 pagesForest Flower October 2018RAGUNATH PNo ratings yet
- Jurnal Semi FowlerDocument6 pagesJurnal Semi FowlerHartina RolobessyNo ratings yet
- Ace of Spades + Outlaw 125 2019Document85 pagesAce of Spades + Outlaw 125 2019Nelson RodrigoNo ratings yet
- Hirschsprung's Disease - AthigamanDocument128 pagesHirschsprung's Disease - Athigamanprived100% (4)
- Air Tunnels: Submitted By: Priyanka Sinha SK MD Sibli Akram Ananya Sreyansri NandaDocument8 pagesAir Tunnels: Submitted By: Priyanka Sinha SK MD Sibli Akram Ananya Sreyansri NandaPriyanka SinhaNo ratings yet